Suprascapular Nerve Decompression PDF¶
Rehabilitation after isolated arthroscopic suprascapular nerve decompression, with honest framing of nerve recovery.
This protocol covers the rehabilitation after an isolated arthroscopic suprascapular nerve decompression with Dr Kieran Hirpara at Mater Private Hospital Rockhampton — the release of the nerve at the suprascapular notch and/or the spinoglenoid notch, without any other repair. Bring this page or its PDF to your first physiotherapy visit so your rehabilitation stays coordinated. Your rehabilitation is progressed individually by your physiotherapist through the phases below, depending on how your shoulder recovers.
Important — please read first. Suprascapular nerve decompression is often performed together with a rotator cuff repair. This protocol is for an isolated decompression only. If your operation also included a rotator cuff repair, follow the rotator cuff repair protocol instead — the repaired tendon sets a slower pace, and that protocol takes precedence over this one. If you are not sure which operation you had, ask the rooms before you start.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
When the nerve is released on its own, there is no tendon repair that needs protecting, so rehabilitation can move quickly. The sling is worn only for comfort and only briefly — usually for about the first week, and up to two weeks at most — and it is left off as much as possible once the shoulder settles. Gentle movement begins early, as comfort allows, and most people are back to their normal daily activities within a few weeks.
Recovery of the nerve itself follows its own timeline, separate from the movement of the shoulder. The operation relieves the pressure on the nerve; the pain from that pressure often eases relatively quickly. Recovery of muscle strength and bulk in the muscles the nerve supplies (the supraspinatus and infraspinatus, which sit on the shoulder blade) is slower and works on a scale of months. How fully strength and muscle bulk return varies from person to person — in some people recovery is complete, in others it is partial, and a longstanding nerve problem may not recover fully. Your physiotherapy includes specific work to reactivate these muscles as the nerve recovers. Your physiotherapist and the practice will guide you on what to expect in your case.
Phase I — Early movement (Week 0–2)¶
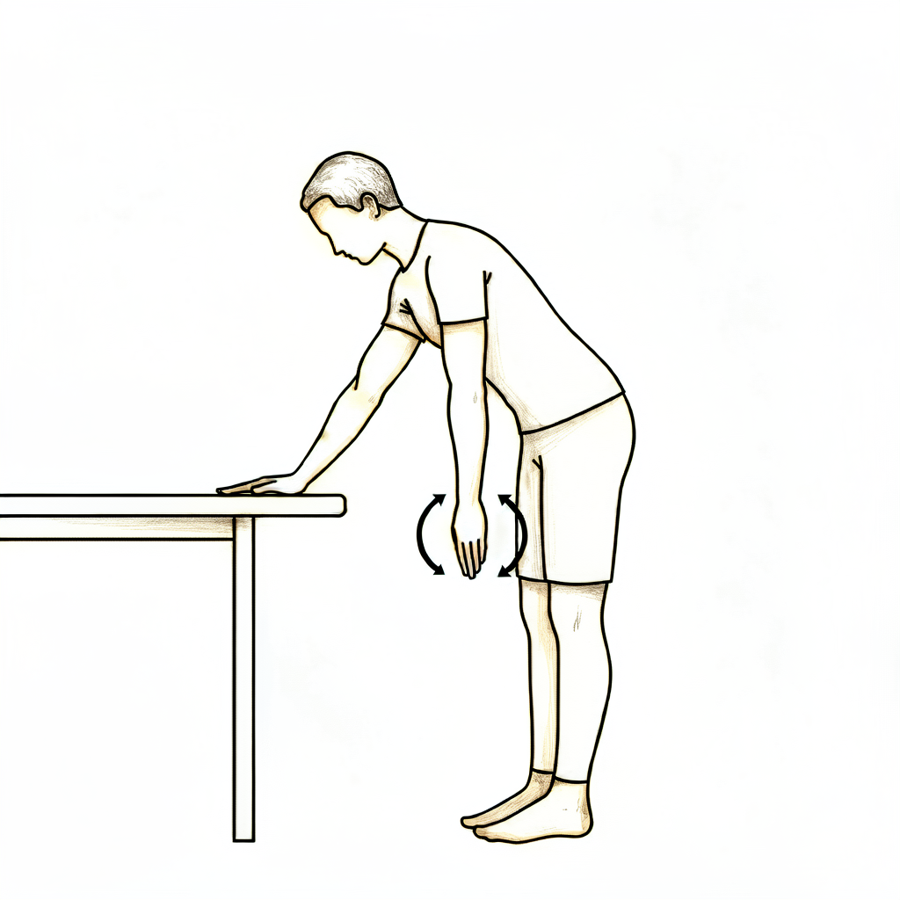
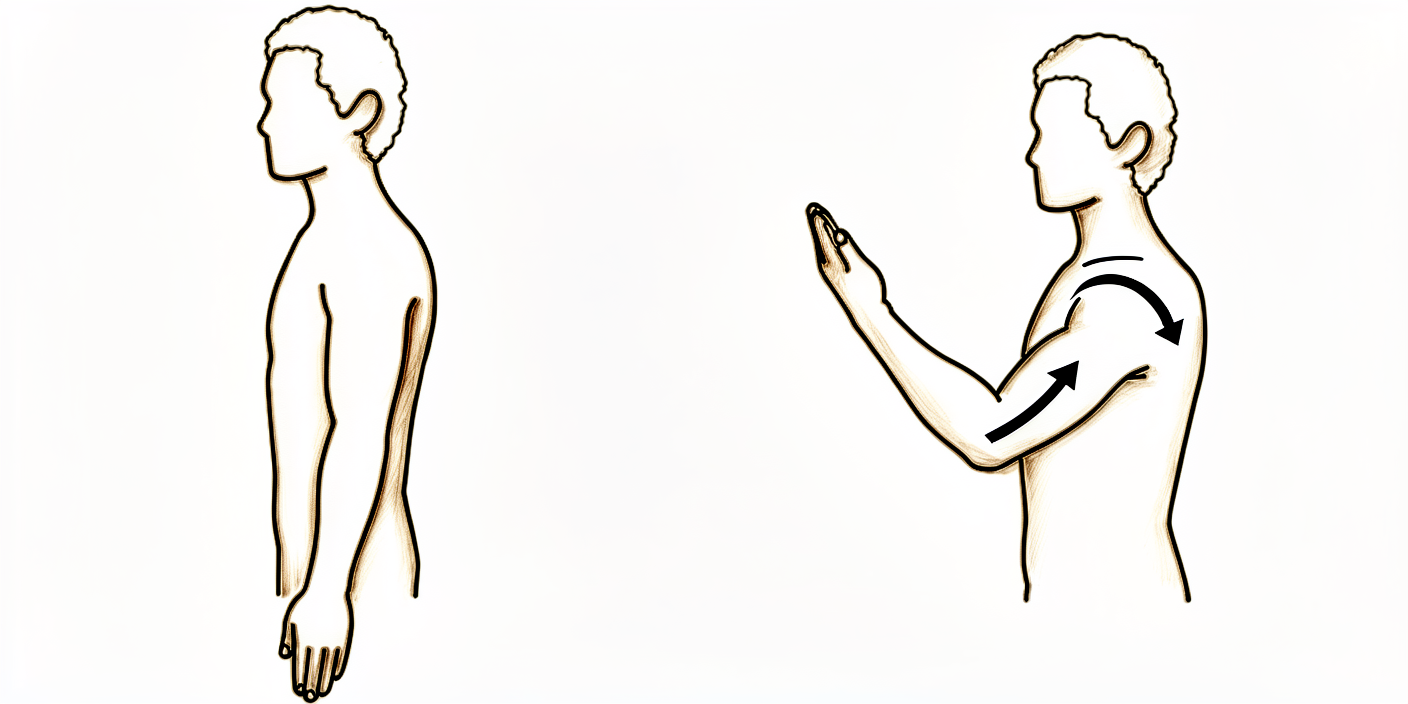
Pendulum exercise
Bend forward at the waist and let the operated arm hang gently away from the body. Let the arm swing in small, relaxed circles — the movement comes from your body, not the shoulder muscles. Stay within a comfortable, pain-free range.
As guided by your physiotherapist
Kieran Hirpara 4.0
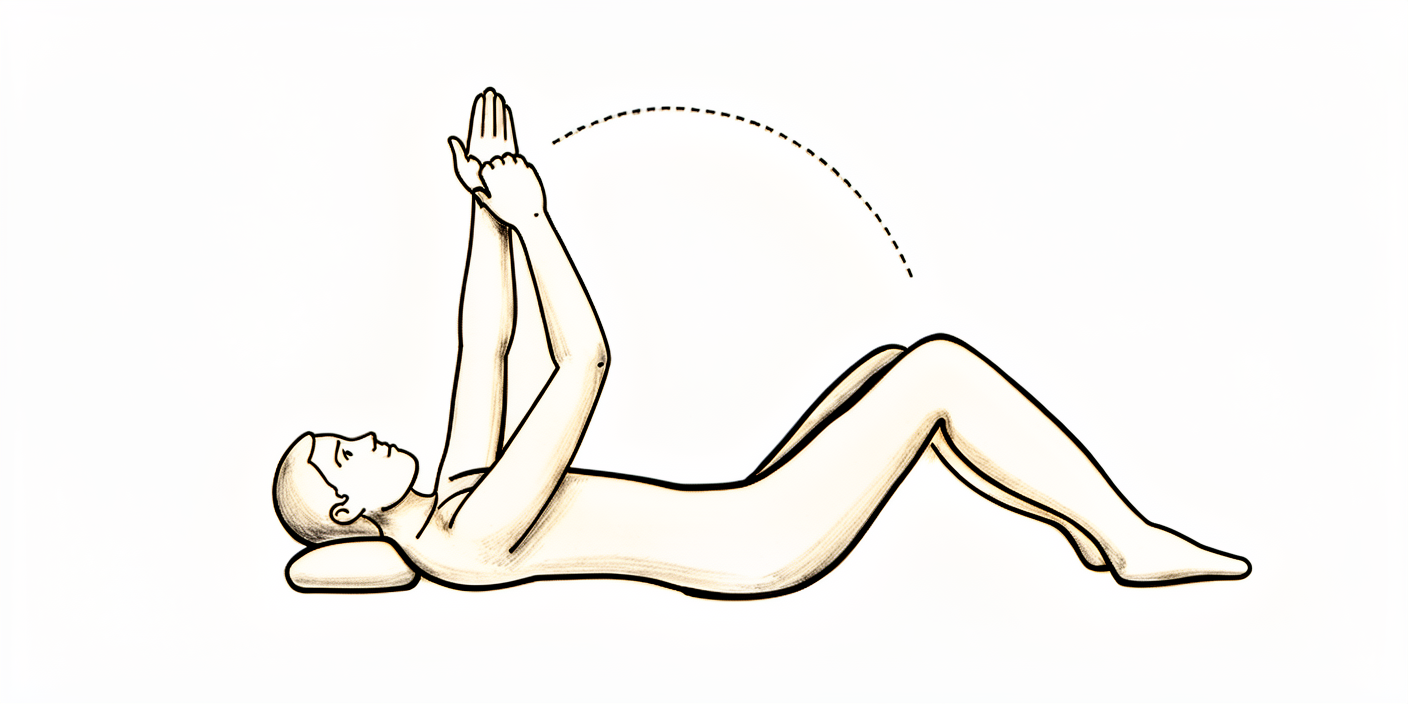
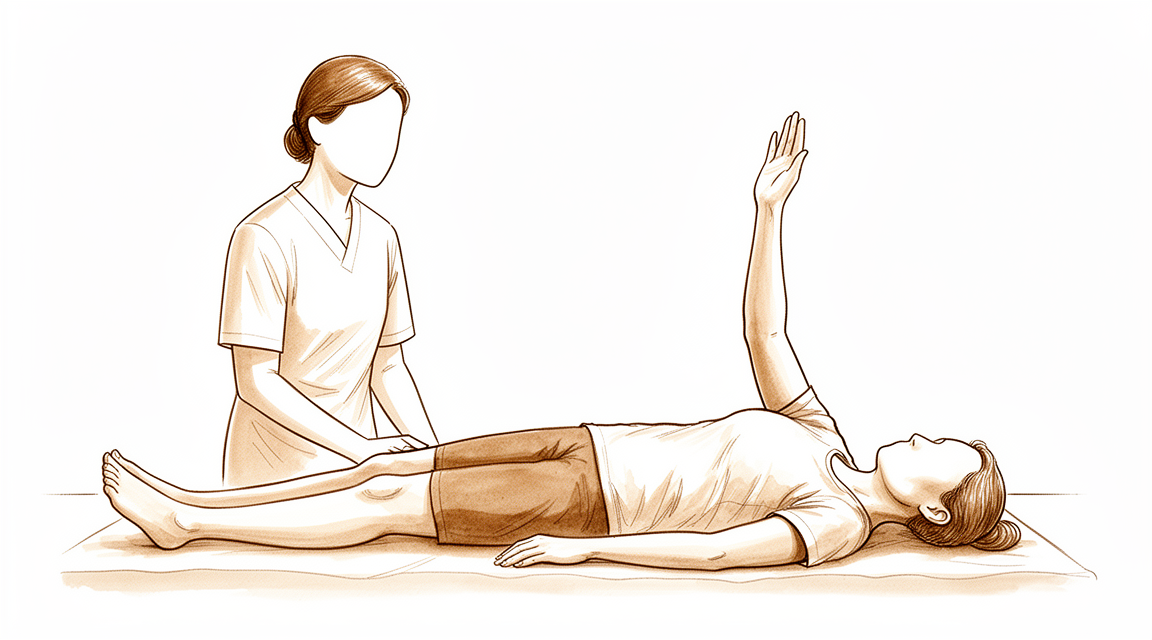
Assisted elevation (lying)
Lie on your back and use your good arm to help lift the operated arm upwards, then lower it back down with the good arm still helping. Move only within a comfortable, pain-free range — gentle, early movement is the aim, not range at any cost.
As guided by your physiotherapist
Kieran Hirpara 4.0
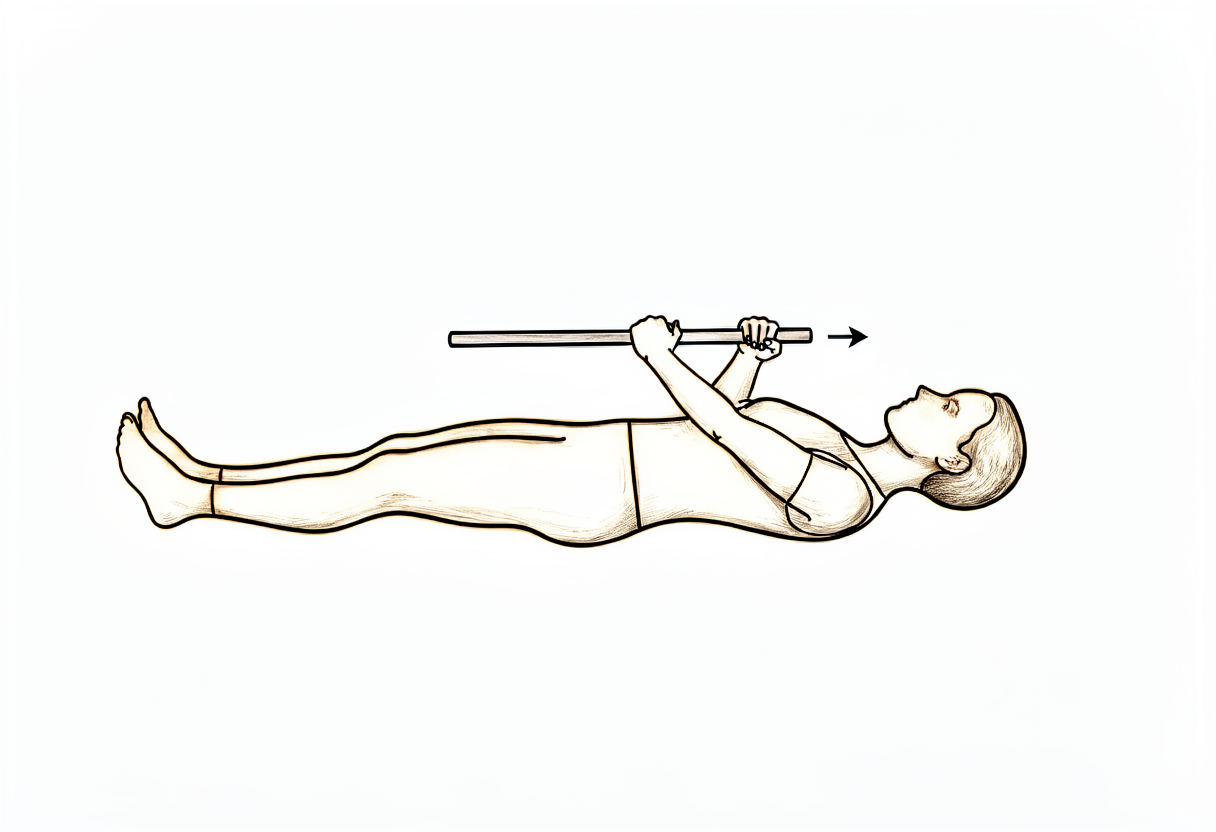
Wand-assisted external rotation
Lie on your back holding a stick or cane in both hands with the elbows bent to right angles and tucked at your sides. Use the good arm to push the operated forearm gently outward, away from the body, then return. Keep the movement comfortable and pain-free.
As guided by your physiotherapist
Kieran Hirpara 4.0
Elbow bends
Bend and straighten the elbow through its full range. Keep the hand, wrist and elbow moving from the start so the rest of the arm stays supple while the shoulder settles.
As guided by your physiotherapist
Kieran Hirpara 4.0
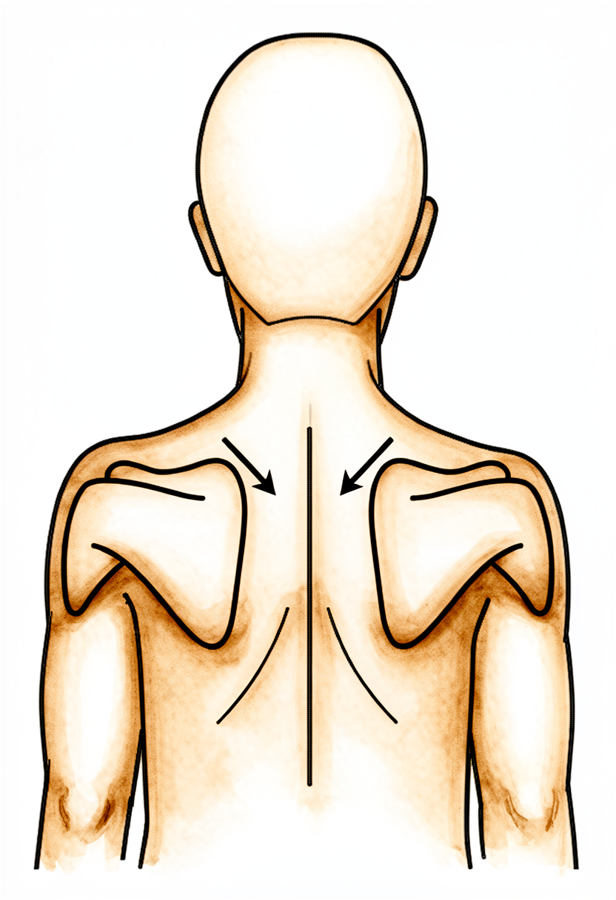
Scapular setting
Sitting or standing tall, gently draw your shoulder blades back together and down, away from your ears. Hold for a few seconds, then relax. Do this as comfort allows in the early days.
As guided by your physiotherapist
Kieran Hirpara 4.0
The first aim is comfort and gentle, early movement. The sling is for comfort only and should be left off as much as possible once the shoulder settles — you do not need to sleep in it. Do not drive while you are wearing the sling. Take your pain relief regularly in the early days so you can begin moving the arm. Keep your hand, wrist and elbow moving from the start, and begin gentle shoulder movement within a comfortable range as advised.
For your physiotherapist:
Goals
- Comfort and wound protection
- Early gentle range of motion within pain-free limits
- Maintain hand, wrist and elbow movement
Management
- Sling for comfort only, typically through about postoperative day 7 (up to two weeks if needed for comfort), weaned as symptoms allow
- Early gentle range of motion as comfort allows — pendulums, passive and active-assisted elevation, external and internal rotation, and elbow flexion/extension
- Isometric deltoid setting and scapular setting as comfortable
- Analgesia before exercise; cryotherapy for pain relief as needed
Precautions
- Keep early movement within a comfortable, pain-free range
- No heavy lifting, forceful pushing or pulling
- No driving while the sling is being worn
Criteria to progress
- Comfortable, settling pain
- Wound healing satisfactorily
- Early range of motion tolerated
Phase II — Range and muscle reactivation (Week 2–6)¶
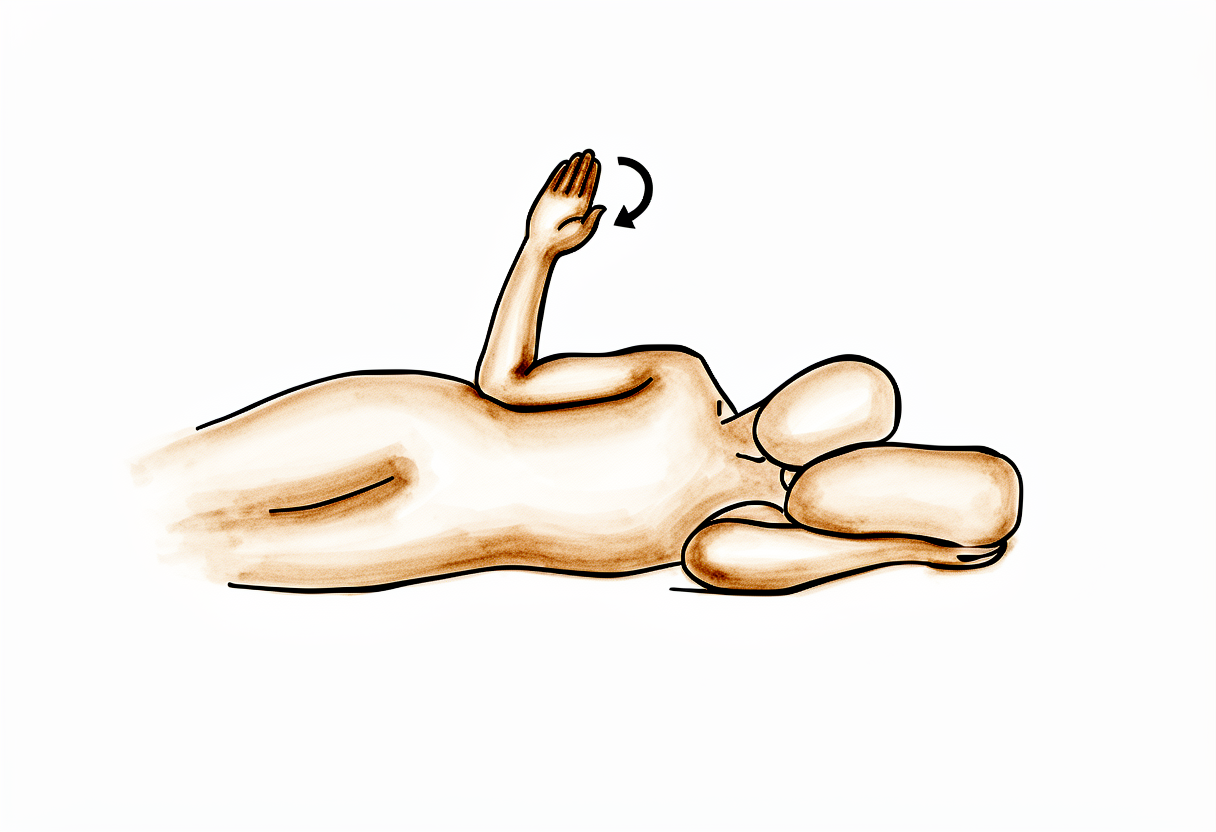
Side-lying external rotation
Lie on your non-operated side with the top elbow bent to a right angle and tucked against your body. Keeping the elbow at your side, rotate the forearm up towards the ceiling, then lower with control. Pain-free external rotation like this helps reactivate the muscles the nerve supplies.
As guided by your physiotherapist
Kieran Hirpara 4.0
With the sling discarded, this phase restores full movement and begins light strengthening, including specific work to reactivate the supraspinatus and infraspinatus as the nerve recovers. Most people return to their normal daily activities during this phase. Progress is guided by comfort, not the calendar.
For your physiotherapist:
Goals
- Full active range of motion in all planes
- Begin light strengthening and rotator cuff (supraspinatus/infraspinatus) reactivation
- Independence with activities of daily living
Management
- Progress to full active range of motion in all directions
- Begin light strengthening from around week 2 — isometrics progressing to elastic-band work for the rotator cuff, deltoid and scapular stabilisers, low load and higher repetitions
- Particular attention to pain-free external rotation and to reactivating the supraspinatus and infraspinatus as the nerve recovers
- Graduated return to normal daily activities, typically by around four weeks
Precautions
- Strengthening stays within a comfortable range and should not provoke pain that lingers
- Avoid forceful pushing, pulling and heavy lifting while strength recovers
- Expect strength to return gradually — reactivation work is paced to the nerve's recovery, not forced
Criteria to progress
- Full, or near-full, pain-free active range of motion
- Light strengthening tolerated without flare-up
Phase III — Strengthening and return to activity (Week 6–12 and beyond)¶
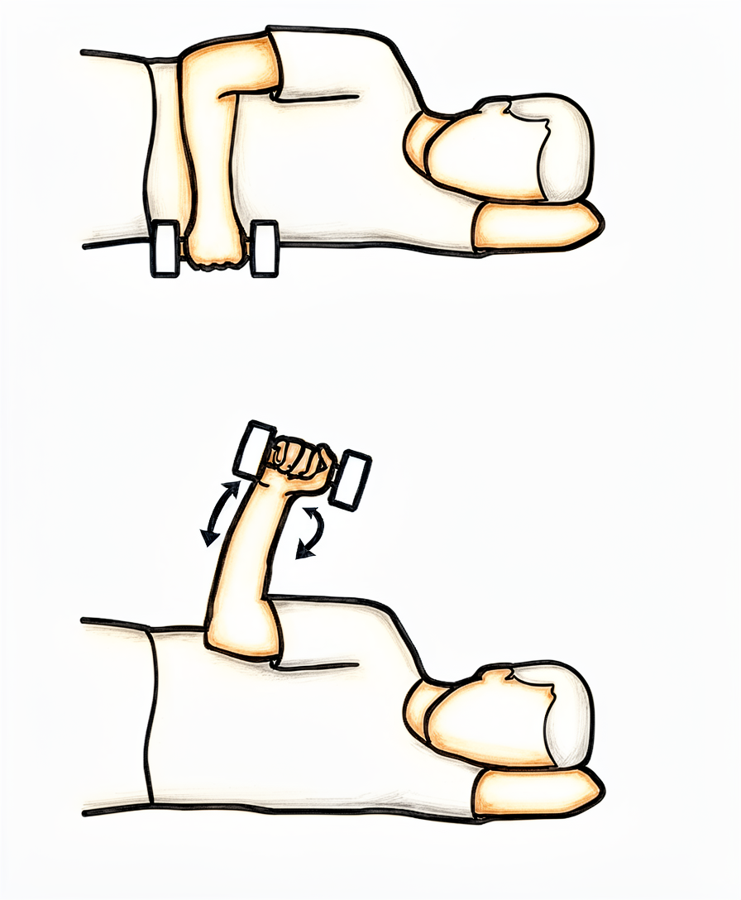
Side-lying external rotation with weight
From around week 12, the same side-lying rotation is done holding a light weight: elbow bent to a right angle and tucked at the side, rotate the forearm up towards the ceiling, then lower slowly. This isolates the muscles the nerve supplies as it recovers — progress is paced to the nerve, not forced.
As guided by your physiotherapist
Kieran Hirpara 4.0
From around six weeks, strengthening progresses without specific restriction, building towards a return to overhead tasks, heavier work and sport. Isolated strengthening of the supraspinatus and infraspinatus is advanced as the nerve continues to recover, which typically continues over several months.
For your physiotherapist:
Goals
- Full strengthening without restriction
- Graduated return to overhead activity, heavier work and sport
- Continued recovery of rotator cuff strength as the nerve recovers
Management
- From around week 6, progress to full strengthening, including closed-chain and progressive resistance work
- From around week 12, advance isolated supraspinatus and infraspinatus strengthening
- Stage the return to overhead work and sport — full return to overhead activity is often reached by around four to six weeks for lighter tasks, with a graduated return to sport over the following weeks to months as strength allows and once pain-free
- Continue a maintenance programme as the nerve and muscles keep recovering
Precautions
- Progression remains symptom-guided
- Strength and muscle bulk in the affected muscles may keep recovering over several months, and recovery may be partial — pace expectations accordingly and avoid overstressing while strength is incomplete
After your protocol¶
The phases above are adapted from published technique papers and clinical studies on arthroscopic suprascapular nerve decompression (the sources are listed below). The week ranges are typical rather than fixed, and your ongoing rehabilitation is guided individually by your physiotherapist, working with the practice, based on how your shoulder and the nerve recover. This page works alongside the practice's general recovery advice — see managing post-operative pain and wound care. For the operation itself and the condition it treats, see suprascapular nerve decompression.
References
- Plancher KD, Evely TB, Brite JE, Briggs KK, Petterson SC. Endoscopic/arthroscopic decompression of the suprascapular nerve at the spinoglenoid notch: indications and surgical technique. JSES Rev Rep Tech. 2021;1(3):198-206.
- Harkin WE, Kerzner B, Scanaliato J, et al. Open Suprascapular Nerve Decompression at the Spinoglenoid Notch. Arthrosc Tech. 2024;13(9):103051.
- Brzoska R, Laprus H, Klaptocz P, et al. Arm Function After Arthroscopic Decompression of the Suprascapular Nerve at the Spinoglenoid Notch and Suprascapular Notch in Volleyball Players. Orthop J Sports Med. 2023;11(2):23259671221147892.
- Feinberg JH, Mehta P, Gulotta LV, et al. Electrodiagnostic evidence of suprascapular nerve recovery after decompression. Muscle Nerve. 2019;59(2):247-249.