AC Joint Stabilisation PDF Evidence¶
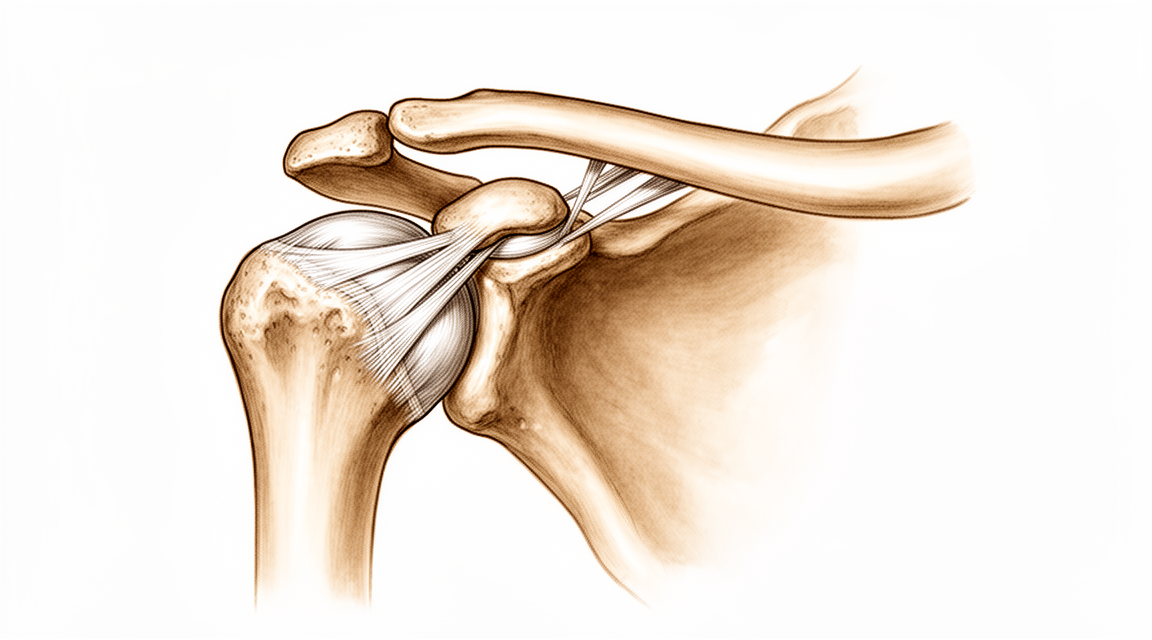
Surgical reconstruction for high-grade AC joint dislocation (Rockwood III-VI).
Why this operation has been suggested¶
This operation repairs the ligaments that hold your collarbone to your shoulder blade after a severe separation. Your surgeon likely suggested it because you have a high-grade injury where the bones are significantly displaced and the joint is unstable. While mild separations usually heal with a sling, surgery is recommended for severe cases to prevent lasting pain and limited movement.
The main goal of this procedure is to restore stability to your shoulder so you can return to daily activities and work without pain. It is typically offered when non-surgical options have failed or when the injury is too severe to heal on its own. By fixing the joint, the operation aims to relieve pain and help you regain full function.
Before the operation¶
You will need to fast for several hours before your surgery and stop certain medications as your surgeon advises. Please arrange for someone to drive you home and bring a list of all current medicines. You may need X-rays, an MRI, blood tests, or an anaesthetic review to check your health and plan the procedure. Your surgeon will use a single open incision over the shoulder to stabilize the joint. This approach allows direct access to repair the ligaments. Wear comfortable clothing to your appointment. Most patients with this injury have a bump on the top of the shoulder that may need fixing.
On the day¶
You will arrive at the hospital and meet your surgeon and the anaesthetist. This operation is done under general anaesthetic combined with a regional nerve block. You will be fully asleep for the operation, and the block — an injection that numbs the nerves supplying the arm before you wake up — provides pain relief for the first 12 to 24 hours after surgery. The anaesthetist will meet you before the operation and talk you through both parts.
Your surgeon will perform the procedure through a single conventional incision over the operative site. You will then be moved to the recovery area to wake up. You may feel sleepy or groggy as the anaesthetic wears off, but your team will monitor you closely until you are stable.
What the operation involves¶
Your surgeon will make a single cut over the front of your shoulder, extending from the collarbone toward the breastbone. This approach, often called a 'bra-strap' incision, gives your surgeon a clear view of the joint while protecting the surrounding soft tissues.
Inside, your surgeon will repair the torn ligaments that hold your collarbone in place. For high-grade injuries, this involves fixing both the top joint and the deeper ligaments connecting the collarbone to the shoulder blade. If you are having surgery for arthritis, your surgeon will remove a small piece of bone from the end of the collarbone. This piece is usually between 5 to 10 mm long to stop the bones from rubbing together.
Once the repair is complete, your surgeon will close the cut with stitches. The skin is then covered with a dressing to protect the area while it heals.
After the operation¶
You will wake up in the recovery ward. Your surgeon will manage your pain using standard methods. You will have a dressing over your incision and wear an arm sling. The sling is usually used for about 1 week for type I injuries or 2 to 3 weeks for type II injuries. You can usually go home the same day or after one night. You must have someone stay with you for the first 24 hours. You will begin moving your arm gently soon after surgery, but avoid heavy lifting or contact sports for about 2 to 3 months.
Recovery¶
In the first few days, you will feel soreness and swelling around your shoulder. This is normal as your body heals. Your surgeon may recommend a sling to support your arm and limit movement. You will likely sleep with your upper body slightly elevated to reduce discomfort.
As the swelling settles, your physiotherapist will guide you through gentle exercises. These movements help restore your shoulder's range of motion without straining the repair. You will gradually learn to use your arm for daily tasks like eating or dressing. Heavy lifting and contact sports are not allowed until your surgeon confirms your shoulder is stable.
Your recovery journey is unique. While most people regain full function, the pace depends on your body and how well you follow your plan. Your surgeon and physiotherapist will monitor your progress and adjust your exercises as needed. You will know you are ready for the next step when you can move your arm without pain.
What can go wrong¶
Most patients do well, but problems can occasionally happen. Your surgeon and the team monitor you closely to spot any issue early.
You might notice a deep, throbbing pain in your shoulder that does not ease with simple painkillers. This can happen months or even years after your injury or surgery. If this pain persists, call your surgeon's clinic to discuss your next steps.
Some patients feel a clicking or grinding sensation in the joint. You might also notice the bump on top of your shoulder looks different or feels unstable. This could mean the joint has slipped back out of place. Contact your surgeon immediately if you see this change.
You may experience redness, warmth, or swelling around the incision site. If these signs spread or you develop a fever, go to the emergency department right away.
If you have persistent symptoms that do not improve with rest, your surgeon might discuss further treatment. This could involve another procedure to fix the joint.
The complications table on this page lists typical rates if you want the specifics.
When to call us¶
Call us if you have a fever, increasing redness or discharge from your wound, or sudden severe pain. Go to emergency immediately if you notice swelling in your calf, shortness of breath, loss of sensation, or if you cannot move your arm. These signs may indicate infection, a blood clot, or nerve issues that need urgent care.
Evidence & references
title: "AC Joint Stabilisation" slug: ac-joint-stabilisation region: shoulder audience: patient mesh_terms: [] article_count: 129 model_used: qwen3.5-35b-a3b-q8 generated_at: '2026-05-18T13:55:12+00:00' key_articles: [] synthesis_version: "v2" verifier_status: skipped
Overview¶
- AC joint separation is a common injury with an unknown incidence [1].
- Injury results in progressive disruption of the ligamentous support of the AC joint, beginning with the capsular ligaments and progressing to the CC ligaments [1].
- The mechanism of injury is usually direct trauma resulting from a fall on the point of the shoulder [1].
- Indirect injuries of the AC joint are rare [1].
- Higher grade AC joint injuries result in prominence of the distal clavicle [1].
- Localized bruising, swelling, and tenderness are present in acute AC joint injuries [1].
- The sternoclavicular joint should be evaluated for swelling, deformity, and tenderness in AC joint injuries [1].
- Range of motion and rotator cuff strength typically are normal in chronic AC joint injuries but may be limited in acute injuries secondary to pain [1].
- The ability to reduce the deformity with manual pressure can help differentiate nonsurgical versus surgical treatment for higher grade AC joint injuries [1].
- Horizontal plane translation of the distal clavicle should be assessed manually and compared with the opposite shoulder [1].
- A complete neurologic examination of the upper extremity should be performed to rule out brachial plexus injuries in AC joint trauma [1].
- Scapular dyskinesis can be seen with AC joint injuries [1].
- Plain radiographs for AC joint evaluation include an AP view of the clavicle, a caudal tilt view, and an axillary view [1].
- The axillary view is needed to rule out posterior translation of the distal clavicle [1].
- In a normal AC joint, the anterior aspect of the clavicle should lie in the same plane as the anterior aspect of the acromion [1].
- The normal coracoclavicular distance between the superior aspect of the coracoid and the inferior clavicle should be between 11 to 13 mm [1].
- A fracture of the base of the coracoid process should be ruled out in AC joint injuries [1].
- A coracoid fracture can result in superior displacement of the clavicle but an intact CC distance, creating a functionally equivalent AC joint separation [1].
- A Zanca view is a modified, underpenetrated AP view with a cephalic tilt of 10° to 15° that gives excellent detail of the distal clavicle [1].
- Weighted views include bilateral AP views with a weight tied to the wrists in relaxed standing [1].
- Weighted views help distinguish between type II and type III separations but rarely are indicated and often are not clinically helpful [1].
- Type I AC joint injury is an AC ligament sprain with intact CC ligaments and normal radiographic CC distance [1].
- Type II AC joint injury is an AC ligament rupture with sprained but intact CC ligaments and normal radiographic CC distance [1].
- Type III AC joint injury involves disruption of the AC and CC ligaments, characterized by increased CC distance and superior displacement of the clavicle of up to 100% of the clavicle width [1].
- The deformity in type III AC joint injuries is reducible [1].
- A modification of type III injuries has been proposed consisting of type IIIA (horizontally stable) and type IIIB (horizontally unstable) [1].
- Type IV AC joint injury involves disruption of the AC and CC ligaments with posterior displacement of the clavicle, increased CC distance, and the distal clavicle herniated into or through the deltotrapezial fascia [1].
- The deformity in type IV AC joint injuries is not reducible [1].
- Type V AC joint injury involves disruption of the AC and CC ligaments with greater than 100% superior displacement of the clavicle and a markedly increased CC distance [1].
- The deformity in type V AC joint injuries is usually not reducible because of herniation through the deltotrapezial fascia [1].
- Type VI AC joint injury involves disruption of the AC and CC ligaments with inferior clavicle displacement, where the distal clavicle lies under the acromion or coracoid process [1].
- Type VI AC joint injuries are rare [1].
- Nonsurgical treatment is recommended for type I and II AC joint injuries [1].
- Good functional outcomes can be expected with nonsurgical treatment for type I and II AC joint injuries [1].
- Sling immobilization is followed by gradual active ROM exercises and stretching, then strengthening as tolerated for type I and II AC joint injuries [1].
- Most patients regain full shoulder function within 4 to 6 weeks after type I or II AC joint injury [1].
- Patients with AC joint injuries are at increased risk for painful AC joint arthritis [1].
- Between 30% and 50% of young, very active patients will have mild to moderate residual pain at the AC joint [1].
- The recommended treatment for type III AC joint injuries is controversial and depends on patient age and activity level [1].
- Multiple retrospective comparative studies have shown good clinical results and return to sport with nonsurgical treatment for type III injuries and no advantage from surgery [1].
- Criticisms of studies comparing surgical and nonsurgical treatment for type III injuries primarily relate to the use of antiquated surgical techniques in the surgical groups [1].
- Meta-analysis and systematic reviews demonstrate similar outcomes for type III separations managed nonsurgically and surgically [1].
- Nonsurgical treatment for type III AC joint injuries resulted in quicker recovery and return to work [1].
- Surgical treatment for type III AC joint injuries resulted in an increase in complications [1].
- One prospective, randomized trial of type III and V injuries showed better results with nonsurgical treatment when clavicle displacement was less than 2 cm [1].
- One prospective, randomized trial of type III and V injuries showed better results with surgical management when the clavicle was displaced more than 2 cm [1].
- Nonsurgical treatment for type IV, V, and VI AC joint injuries likely results in substantial residual pain and limited function [1].
- Outcomes studies for nonsurgical treatment of type IV, V, and VI AC joint injuries are limited [1].
- Surgical treatment is recommended for most patients with type IV, V, and VI AC joint injuries [1].
- Surgery is indicated for most acute type IV, V, and VI AC joint separations [1].
- Surgery can be performed acutely in selected type III separations in younger, physically active patients [1].
- Surgery can be performed acutely in selected type III separations in manual laborers [1].
- Surgery can be performed acutely in selected type III separations in patients with cosmetic concerns [1].
- Surgery can be performed acutely in selected type III separations in patients with chronic injuries who have persistent symptoms [1].
- Surgery is often recommended for patients with type IIIB (horizontally unstable) AC joint separations [1].
- Healing of the CC ligaments is reliable without the need for graft augmentation if adequate reduction and stabilization are achieved in acute surgery less than 3 to 4 weeks following injury [1].
Anatomy & Pathophysiology¶
- AC joint separation is a common injury with an unknown incidence [1].
- The mechanism of injury for AC joint separation is usually direct trauma from a fall on the point of the shoulder [1].
- Indirect injuries to the AC joint are rare [1].
- Injury to the AC joint results in progressive disruption of ligamentous support, beginning with capsular ligaments and progressing to coracoclavicular (CC) ligaments [1].
- Higher grade AC joint injuries result in prominence of the distal clavicle [1].
- Localized bruising, swelling, and tenderness are present in acute AC joint injuries [1].
- The sternoclavicular joint should be evaluated for swelling, deformity, and tenderness in AC joint injuries [1].
- Range of motion and rotator cuff strength are typically normal in chronic AC joint injuries but may be limited in acute injuries secondary to pain [1].
- The ability to reduce the deformity with manual pressure can help differentiate nonsurgical versus surgical treatment for higher grade AC joint injuries [1].
- Horizontal plane translation of the distal clavicle should be assessed manually and compared with the opposite shoulder [1].
- A complete neurologic examination of the upper extremity should be performed to rule out brachial plexus injuries in AC joint trauma [1].
- Scapular dyskinesis can be seen with AC joint injuries [1].
- Plain radiographs for AC joint evaluation include an AP view of the clavicle, a caudal tilt view, and an axillary view [1].
- An axillary view is needed to rule out posterior translation of the distal clavicle [1].
- In a normal shoulder, the anterior aspect of the clavicle should lie in the same plane as the anterior aspect of the acromion [1].
- The normal coracoclavicular distance between the superior aspect of the coracoid and the inferior clavicle should be between 11 to 13 mm [1].
- A fracture of the base of the coracoid process should be ruled out as it can result in superior displacement of the clavicle with an intact CC distance [1].
- A Zanca view is a modified, underpenetrated AP view with a cephalic tilt of 10° to 15° that gives excellent detail of the distal clavicle [1].
- Weighted views include bilateral AP views with a weight tied to the wrists in relaxed standing [1].
- Weighted views help distinguish between type II and type III separations but are rarely indicated and often not clinically helpful [1].
- Type I AC joint injury involves an AC ligament sprain with intact CC ligaments and normal radiographic CC distance [1].
- Type II AC joint injury involves AC ligament rupture with sprained but intact CC ligaments and normal radiographic CC distance [1].
- Type III AC joint injury involves disruption of both AC and CC ligaments, characterized by increased CC distance and superior displacement of the clavicle of up to 100% of the clavicle width [1].
- A modification of type III injuries has been proposed consisting of type IIIA (horizontally stable) and type IIIB (horizontally unstable) [1].
- Type IV AC joint injury involves disruption of AC and CC ligaments with posterior displacement of the clavicle [1].
- In type IV injuries, the distal clavicle is herniated into or through the deltotrapezial fascia and the deformity is not reducible [1].
- Type V AC joint injury involves disruption of AC and CC ligaments with greater than 100% superior displacement of the clavicle [1].
- In type V injuries, the deformity is usually not reducible because of herniation through the deltotrapezial fascia [1].
- Type VI AC joint injury involves disruption of AC and CC ligaments with inferior clavicle displacement [1].
- In type VI injuries, the distal clavicle lies under the acromion or coracoid process [1].
- Type I injury involves AC ligament sprain without injury to CC ligaments, no AC joint widening, and no clavicular displacement [2].
- Type II injuries consist of complete rupture of the AC ligament, CC ligament sprain, widening of the AC joint, and an increase in CC distance by less than 25% compared with the contralateral shoulder [2].
- In type III injuries, the AC and CC ligaments are disrupted, the AC joint is widened, and the CC distance is increased 25% to 100% compared with the contralateral shoulder [2].
- A type IV AC joint separation is diagnosed when the distal clavicle is displaced posteriorly into the trapezius muscle [2].
- Type V injury involves disruption of the deltotrapezial fascia with CC distance increased by more than 100% compared with the contralateral shoulder, and tenting of the overlying skin can result [2].
- Type VI injury involves inferior displacement of the clavicle into the subcoracoid space [2].
- In type I injuries, AC ligaments are sprained, CC ligaments are intact, and the deltotrapezial fascia is intact [2].
- In type II injuries, AC ligaments are disrupted, CC ligaments are sprained, and the deltotrapezial fascia is intact [2].
- In type III injuries, AC ligaments, CC ligaments, and the deltotrapezial fascia are all disrupted [2].
- In type IV injuries, AC ligaments, CC ligaments, and the deltotrapezial fascia are all disrupted [2].
- In type V injuries, AC ligaments, CC ligaments, and the deltotrapezial fascia are all disrupted [2].
- In type VI injuries, AC ligaments are disrupted, CC ligaments are intact, and the deltotrapezial fascia is disrupted [2].
- The horizontal plane stability of the clavicle is provided by the AC ligaments, specifically the posterior and superior portions [3].
- Osteoarthritis of the AC joint is more common with advanced age following degeneration of the intra-articular disk [3].
- Arthritic deterioration of the AC joint starts in early middle age [3].
- AC joint osteoarthritis is more common in patients engaged in repetitive overhead or lifting activities [3].
- Previous low-grade AC joint separations can result in painful arthritis [3].
- The radiographic severity of AC joint arthritis does not always correlate with patient symptoms [3].
- Patients with AC joint osteoarthritis report activity-related pain localized to the AC joint, with occasional radiation anteriorly or along the trapezius [3].
- Pain with heavy lifting or when sleeping on the affected side is reported in AC joint osteoarthritis [3].
- Point tenderness is seen at the AC joint in patients with osteoarthritis [3].
- Pain at the AC joint with terminal elevation and cross-body motion is often seen in osteoarthritis [3].
- Selective injection of anesthetic into the AC joint can confirm the diagnosis of osteoarthritis [3].
- Osteophyte formation, sclerotic reaction, and bone cysts are commonly seen on radiographs of AC joint osteoarthritis [3].
- Bone and joint edema on MRI correlate with AC joint pain [3].
- Distal clavicle osteolysis is a localized hyperemia of the distal clavicle resulting in inflammation, bone resorption, microfractures, and secondary arthritis of the AC joint [3].
- Distal clavicle osteolysis is more common in males [3].
- Distal clavicle osteolysis is seen in younger patients [3].
- Distal clavicle osteolysis is associated with heavy lifting (weight lifters) or repetitive motions [3].
- Injuries to the AC joint constitute 9% of shoulder injuries [6].
- AC joint injuries are often caused by direct trauma to the shoulder or a fall on an outstretched hand [6].
- Younger, physically active athletes are at increased risk for AC joint injuries [6].
- Patients involved in contact and extreme sports, as well as high-risk activities such as skiing and cycling, are at increased risk for AC joint injuries [6].
- The extent of injury to the AC and coracoclavicular ligaments determines the severity of AC joint separation [6].
- The amount and direction of clavicle displacement determines the severity of AC joint separation [6].
Classification¶
- AC joint separation is a common injury with an unknown incidence [1].
- Injury to the AC joint results in progressive disruption of ligamentous support, beginning with capsular ligaments and progressing to coracoclavicular (CC) ligaments [1].
- The mechanism of AC joint injury is usually direct trauma from a fall on the point of the shoulder; indirect injuries are rare [1].
- Higher grade AC joint injuries result in prominence of the distal clavicle [1].
- Localized bruising, swelling, and tenderness are present in acute AC joint injuries [1].
- The sternoclavicular joint should be evaluated for swelling, deformity, and tenderness in AC joint injuries [1].
- Range of motion and rotator cuff strength are typically normal in chronic AC joint injuries but may be limited in acute injuries secondary to pain [1].
- The ability to reduce the deformity with manual pressure can help differentiate nonsurgical versus surgical treatment for higher grade AC joint injuries [1].
- Horizontal plane translation of the distal clavicle should be assessed manually and compared with the opposite shoulder [1].
- A complete neurologic examination of the upper extremity should be performed to rule out brachial plexus injuries in AC joint trauma [1].
- Scapular dyskinesis can be seen with AC joint injuries [1].
- Plain radiographs for AC joint evaluation include an AP view of the clavicle, a caudal tilt view, and an axillary view [1].
- An axillary view is needed to rule out posterior translation of the distal clavicle [1].
- In a normal AC joint, the anterior aspect of the clavicle lies in the same plane as the anterior aspect of the acromion [1].
- The normal coracoclavicular distance (between the superior aspect of the coracoid and the inferior clavicle) is between 11 to 13 mm [1].
- A fracture of the base of the coracoid process should be ruled out as it can result in superior displacement of the clavicle with an intact CC distance, creating a functionally equivalent AC joint separation [1].
- A Zanca view is a modified, underpenetrated AP view with a cephalic tilt of 10° to 15° that gives excellent detail of the distal clavicle [1].
- Weighted views include bilateral AP views with a weight tied to the wrists in relaxed standing [1].
- Weighted views help distinguish between type II and type III AC joint separations but are rarely indicated and often not clinically helpful [1].
- Type I AC joint injury involves an AC ligament sprain with intact CC ligaments and normal radiographic CC distance [1].
- Type II AC joint injury involves AC ligament rupture with sprained but intact CC ligaments and normal radiographic CC distance [1].
- Type III AC joint injury involves disruption of the AC and CC ligaments, characterized by increased CC distance and superior displacement of the clavicle of up to 100% of the clavicle width [1].
- The deformity in type III AC joint injuries is reducible [1].
- A modification of type III injuries has been proposed consisting of type IIIA (horizontally stable) and type IIIB (horizontally unstable) [1].
- Type IV AC joint injury involves disruption of the AC and CC ligaments with posterior displacement of the clavicle [1].
- Type IV AC joint injury is characterized by increased CC distance and the distal clavicle herniated into or through the deltotrapezial fascia [1].
- The deformity in type IV AC joint injuries is not reducible [1].
- Type V AC joint injury involves disruption of the AC and CC ligaments with greater than 100% superior displacement of the clavicle [1].
- Type V AC joint injury is characterized by a markedly increased CC distance [1].
- The deformity in type V AC joint injuries is usually not reducible due to herniation through the deltotrapezial fascia [1].
- Type VI AC joint injury involves disruption of the AC and CC ligaments with inferior clavicle displacement [1].
- Type VI AC joint injuries are rare and result in the distal clavicle lying under the acromion or coracoid process [1].
- In 1963, AC joint injuries were initially classified into types I, II, and III [2].
- The AC joint classification was expanded in 1984 to include types IV, V, and VI [2].
- The classification relies on comparative radiographs of the contralateral shoulder to determine each type [2].
- Type I injury involves AC ligament sprain without injury to the CC ligaments, no AC joint widening, and no clavicular displacement [2].
- Type II injuries consist of complete rupture of the AC ligament, CC ligament sprain, widening of the AC joint, and an increase in CC distance by less than 25% compared with the contralateral shoulder [2].
- In type III injuries, the AC and CC ligaments are disrupted, the AC joint is widened, and the CC distance is increased 25% to 100% compared with the contralateral shoulder [2].
- A type IV AC joint separation is diagnosed when the distal clavicle is displaced posteriorly into the trapezius muscle [2].
- Type V injury is similar to type III except the CC distance is increased by more than 100% compared with the contralateral shoulder due to disruption of the deltotrapezial fascia [2].
- Tenting of the overlying skin can result in type V AC joint injuries [2].
- Type VI injury involves inferior displacement of the clavicle into the subcoracoid space [2].
- In Type I AC joint separation, AC ligaments are sprained, CC ligaments are intact, deltotrapezial fascia is intact, and radiographic CC distance is normal (1.1–1.3 cm) [2].
- In Type II AC joint separation, AC ligaments are disrupted, CC ligaments are sprained, deltotrapezial fascia is intact, radiographic CC distance increases by less than 25%, the AC joint appears widened, and the injury is reducible [2].
- In Type III AC joint separation, AC ligaments are disrupted, CC ligaments are disrupted, deltotrapezial fascia is disrupted, radiographic CC distance increases by 25%–100%, the AC joint appears widened, and the injury is reducible [2].
- In Type IV AC joint separation, AC ligaments are disrupted, CC ligaments are disrupted, deltotrapezial fascia is disrupted, radiographic CC distance is increased, there is posterior clavicle displacement, and the injury is not reducible [2].
- In Type V AC joint separation, AC ligaments are disrupted, CC ligaments are disrupted, deltotrapezial fascia is disrupted, radiographic CC distance increases by 100%–300%, and the injury is not reducible [2].
- In Type VI AC joint separation, AC ligaments are disrupted, CC ligaments are intact, deltotrapezial fascia is disrupted, radiographic CC distance is decreased, and the injury is not reducible [2].
Clinical Presentation¶
- AC joint separation is a common injury with an unknown incidence [1].
- The mechanism of injury for AC joint separation is usually direct trauma from a fall on the point of the shoulder [1].
- Indirect injuries of the AC joint are rare [1].
- Injury to the AC joint results in progressive disruption of ligamentous support, beginning with capsular ligaments and progressing to coracoclavicular (CC) ligaments [1].
- Higher grade AC joint injuries result in prominence of the distal clavicle [1].
- Localized bruising, swelling, and tenderness are present in acute AC joint injuries [1].
- The sternoclavicular joint should be evaluated for swelling, deformity, and tenderness in AC joint injury [1].
- Range of motion and rotator cuff strength are typically normal in chronic AC joint injuries but may be limited in acute injuries secondary to pain [1].
- The ability to reduce the deformity with manual pressure can help differentiate nonsurgical versus surgical treatment for higher grade AC joint injuries [1].
- Horizontal plane translation of the distal clavicle should be assessed manually and compared with the opposite shoulder in AC joint injury [1].
- A complete neurologic examination of the upper extremity should be performed to rule out brachial plexus injuries in AC joint injury [1].
- Scapular dyskinesis can be seen with AC joint injury [1].
- Plain radiographs for AC joint evaluation include an AP view of the clavicle, a caudal tilt view, and an axillary view [1].
- An axillary view is needed to rule out posterior translation of the distal clavicle in AC joint injury [1].
- In a normal shoulder, the anterior aspect of the clavicle should lie in the same plane as the anterior aspect of the acromion [1].
- The normal coracoclavicular distance between the superior aspect of the coracoid and the inferior clavicle should be between 11 to 13 mm [1].
- Fracture of the base of the coracoid process should be ruled out in AC joint injury as it can result in superior displacement of the clavicle with an intact CC distance [1].
- A Zanca view is a modified, underpenetrated AP view with a cephalic tilt of 10° to 15° that gives excellent detail of the distal clavicle [1].
- Weighted views include bilateral AP views with a weight tied to the wrists in relaxed standing [1].
- Weighted views help distinguish between type II and type III AC joint separations but are rarely indicated and often not clinically helpful [1].
- Type I AC joint injury involves an AC ligament sprain with intact CC ligaments and normal radiographic CC distance [1].
- Type II AC joint injury involves AC ligament rupture and sprained but intact CC ligaments with normal radiographic CC distance [1].
- Type III AC joint injury involves disruption of the AC and CC ligaments, increased CC distance, and superior displacement of the clavicle of up to 100% of the clavicle width [1].
- The deformity in type III AC joint injury is reducible [1].
- A modification of type III injuries has been proposed consisting of type IIIA (horizontally stable) and type IIIB (horizontally unstable) [1].
- Type IV AC joint injury involves disruption of the AC and CC ligaments with posterior displacement of the clavicle [1].
- In type IV AC joint injury, the distal clavicle is herniated into or through the deltotrapezial fascia [1].
- The deformity in type IV AC joint injury is not reducible [1].
- Type V AC joint injury involves disruption of the AC and CC ligaments with greater than 100% superior displacement of the clavicle [1].
- Type V AC joint injury is characterized by a markedly increased CC distance [1].
- The deformity in type V AC joint injury is usually not reducible because of herniation through the deltotrapezial fascia [1].
- Type VI AC joint injury involves disruption of the AC and CC ligaments with inferior clavicle displacement [1].
- In type VI AC joint injury, the distal clavicle lies under the acromion or coracoid process [1].
- Type I AC joint injury involves an AC ligament sprain without injury to the CC ligaments and no AC joint widening or clavicular displacement [2].
- Type II AC joint injury consists of complete rupture of the AC ligament, CC ligament sprain, widening of the AC joint, and an increase in CC distance by less than 25% compared with the contralateral shoulder [2].
- Type III AC joint injury involves disruption of the AC and CC ligaments, widened AC joint, and increased CC distance of 25% to 100% compared with the contralateral shoulder [2].
- Type IV AC joint separation is diagnosed when the distal clavicle is displaced posteriorly into the trapezius muscle [2].
- Type V AC joint injury involves disruption of the deltotrapezial fascia and tenting of the overlying skin [2].
- Type VI AC joint injury involves inferior displacement of the clavicle into the subcoracoid space [2].
- In type I AC joint injury, AC ligaments are sprained, CC ligaments are intact, and the deltotrapezial fascia is intact [2].
- In type II AC joint injury, AC ligaments are disrupted, CC ligaments are sprained, and the deltotrapezial fascia is intact [2].
- In type III AC joint injury, AC ligaments, CC ligaments, and the deltotrapezial fascia are all disrupted [2].
- In type IV AC joint injury, AC ligaments, CC ligaments, and the deltotrapezial fascia are all disrupted [2].
- In type V AC joint injury, AC ligaments, CC ligaments, and the deltotrapezial fascia are all disrupted [2].
- In type VI AC joint injury, AC ligaments are disrupted, CC ligaments are intact, and the deltotrapezial fascia is disrupted [2].
- The horizontal plane stability of the clavicle is provided by the AC ligaments, specifically the posterior and superior portions [3].
- Osteoarthritis of the AC joint is more common with advanced age following degeneration of the intra-articular disk [3].
- Arthritic deterioration of the AC joint starts in early middle age [3].
- AC joint osteoarthritis is more common in patients engaged in repetitive overhead or lifting activities [3].
- Previous low-grade AC joint separations can result in painful arthritis [3].
- The radiographic severity of AC joint arthritis does not always correlate with patient symptoms [3].
- Patients with AC joint osteoarthritis report activity-related pain [3].
- Pain from AC joint osteoarthritis is localized to the AC joint, with occasional radiation anteriorly or along the trapezius [3].
- Pain with heavy lifting or when sleeping on the affected side is reported in AC joint osteoarthritis [3].
- Point tenderness is seen at the AC joint in patients with osteoarthritis [3].
- Horizontal stability should be assessed in patients with AC joint osteoarthritis [3].
- Pain at the AC joint with terminal elevation and cross-body motion is often seen in osteoarthritis [3].
- Selective injection of anesthetic into the AC joint can confirm the diagnosis of AC joint osteoarthritis [3].
- Radiographs for AC joint osteoarthritis include an AP view and/or a Zanca view of the shoulder [3].
- Osteophyte formation, sclerotic reaction, and bone cysts are commonly seen in AC joint osteoarthritis on radiographs [3].
- Bone and joint edema on MRI correlate with AC joint pain [3].
- Distal clavicle osteolysis is more common in males [3].
- Distal clavicle osteolysis is seen in younger patients [3].
- Distal clavicle osteolysis is associated with heavy lifting or repetitive motions [3].
- Examination findings for distal clavicle osteolysis include localized pain, swelling, and tenderness similar to those seen in symptomatic AC joint arthritis [3].
- The normal CC distance on an AP radiograph should be less than 11 to 13 mm [3].
Investigations¶
- AC joint separation is a common injury with an unknown incidence [1].
- The mechanism of injury for AC joint separation is usually direct trauma from a fall on the point of the shoulder, while indirect injuries are rare [1].
- Higher grade AC joint injuries result in prominence of the distal clavicle [1].
- Localized bruising, swelling, and tenderness are present in acute AC joint injuries [1].
- The sternoclavicular joint should be evaluated for swelling, deformity, and tenderness during AC joint examination [1].
- Range of motion and rotator cuff strength are typically normal in chronic AC joint injuries but may be limited in acute injuries secondary to pain [1].
- The ability to reduce the deformity with manual pressure can help differentiate nonsurgical versus surgical treatment for higher grade AC joint injuries [1].
- Horizontal plane translation of the distal clavicle should be assessed manually and compared with the opposite shoulder [1].
- A complete neurologic examination of the upper extremity should be performed to rule out brachial plexus injuries in AC joint trauma [1].
- Scapular motion should be carefully assessed as scapular dyskinesis can be seen with AC joint injuries [1].
- Plain radiographs for AC joint evaluation include an AP view of the clavicle, a caudal tilt view, and an axillary view [1].
- An axillary view is needed to rule out posterior translation of the distal clavicle [1].
- On an axillary view, the anterior aspect of the clavicle should lie in the same plane as the anterior aspect of the acromion [1].
- The normal coracoclavicular distance between the superior aspect of the coracoid and the inferior clavicle should be between 11 to 13 mm [1].
- A fracture of the base of the coracoid process should be ruled out as it can result in superior displacement of the clavicle with an intact CC distance [1].
- A Zanca view is a modified, underpenetrated AP view with a cephalic tilt of 10° to 15° that gives excellent detail of the distal clavicle [1].
- Weighted views include bilateral AP views with a weight tied to the wrists in relaxed standing [1].
- Weighted views help distinguish between type II and type III AC joint separations but are rarely indicated and often not clinically helpful [1].
- Type I AC joint injury involves an AC ligament sprain with intact CC ligaments and normal radiographic CC distance [1].
- Type II AC joint injury involves AC ligament rupture and sprained but intact CC ligaments with normal radiographic CC distance [1].
- Type III AC joint injury involves disruption of the AC and CC ligaments, increased CC distance, and superior displacement of the clavicle of up to 100% of the clavicle width [1].
- A modification of type III injuries has been proposed consisting of type IIIA (horizontally stable) and type IIIB (horizontally unstable) [1].
- Type IV AC joint injury involves disruption of the AC and CC ligaments with posterior displacement of the clavicle, increased CC distance, and a deformity that is not reducible [1].
- Type V AC joint injury involves disruption of the AC and CC ligaments with greater than 100% superior displacement of the clavicle, a markedly increased CC distance, and a deformity usually not reducible due to herniation through the deltotrapezial fascia [1].
- Type VI AC joint injury involves disruption of the AC and CC ligaments with inferior clavicle displacement, where the distal clavicle lies under the acromion or coracoid process [1].
- Type I AC joint injury involves an AC ligament sprain without injury to the CC ligaments, no AC joint widening, and no clavicular displacement [2].
- Type II AC joint injury consists of complete rupture of the AC ligament, CC ligament sprain, widening of the AC joint, and an increase in CC distance by less than 25% compared with the contralateral shoulder [2].
- Type III AC joint injury involves disruption of the AC and CC ligaments, widened AC joint, and an increase in CC distance of 25% to 100% compared with the contralateral shoulder [2].
- Type IV AC joint separation is diagnosed when the distal clavicle is displaced posteriorly into the trapezius muscle [2].
- Type V AC joint injury involves a CC distance increased by more than 100% compared with the contralateral shoulder due to disruption of the deltotrapezial fascia, with tenting of the overlying skin possible [2].
- Type VI AC joint injury involves inferior displacement of the clavicle into the subcoracoid space [2].
- The horizontal plane stability of the clavicle is provided by the AC ligaments, specifically the posterior and superior portions [3].
- The normal CC distance on an AP radiograph should be less than 11 to 13 mm [3].
- Radiographic severity of AC joint arthritis does not always correlate with patient symptoms [3].
- Patients with AC joint osteoarthritis report activity-related pain localized to the AC joint, with occasional radiation anteriorly or along the trapezius [3].
- Pain with heavy lifting or when sleeping on the affected side is reported in patients with AC joint osteoarthritis [3].
- Point tenderness is seen at the AC joint in patients with osteoarthritis [3].
- Pain at the AC joint with terminal elevation and cross-body motion is often seen in patients with osteoarthritis [3].
- Selective injection of anesthetic into the AC joint can confirm the diagnosis of AC joint pathology [3].
- An AP view and/or a Zanca view of the shoulder provides good visualization of the AC joint for osteoarthritis evaluation [3].
- Osteophyte formation, sclerotic reaction, and bone cysts are commonly seen on radiographs of AC joint osteoarthritis [3].
- Bone and joint edema on MRI correlate with AC joint pain [3].
- Distal clavicle osteolysis is more common in males [3].
- Distal clavicle osteolysis is seen in younger patients [3].
- Distal clavicle osteolysis is associated with heavy lifting or repetitive motions [3].
- Examination findings for distal clavicle osteolysis include localized pain, swelling, and tenderness similar to those seen in symptomatic AC joint arthritis [3].
Treatment¶
- Nonsurgical treatment is recommended for Rockwood type I and II AC joint separations [1].
- Good functional outcomes can be expected with nonsurgical treatment of type I and II injuries [1].
- Sling immobilization is followed by gradual active range of motion exercises, stretching, and strengthening as tolerated for type I and II injuries [1].
- Most patients regain full shoulder function within 4 to 6 weeks following nonsurgical treatment of type I and II injuries [1].
- Patients with type I and II injuries are at increased risk for painful AC joint arthritis [1].
- Between 30% and 50% of young, very active patients will have mild to moderate residual pain at the AC joint after type I or II injuries [1].
- Retrospective studies report persistent symptoms in up to 40% to 50% of patients at 1, 6, and 10 years after type I or II injuries [4].
- The arm sling is typically used for approximately 1 week in type I injuries and for 2 to 3 weeks in type II AC joint separations [4].
- Patients should refrain from contact sports or heavy lifting for approximately 2 to 3 months until full, painless shoulder range of motion is restored [4].
- No evidence supports early surgical management for type I or type II AC joint separations [4].
- Distal clavicle resection, either arthroscopic or open, can provide a solution for patients with persistent AC joint inflammation, osteoarthritis, or distal clavicle osteolysis following failed nonsurgical treatment of type I or II injuries [4].
- The recommended treatment for type III injuries is controversial and depends on patient age and activity level [1].
- Multiple retrospective comparative studies show good clinical results and return to sport with nonsurgical treatment of type III injuries, with no advantage from surgery [1].
- Meta-analyses and systematic reviews demonstrate similar outcomes for type III separations managed nonsurgically and surgically [1].
- Nonsurgical treatment of type III injuries results in quicker recovery and return to work compared to surgical treatment [1].
- Surgical treatment of type III injuries results in an increase in complications compared to nonsurgical treatment [1].
- One prospective randomized trial showed better results with nonsurgical treatment for type III and V injuries when clavicle displacement was less than 2 cm [1].
- One prospective randomized trial showed better results with surgical management for type III and V injuries when the clavicle was displaced more than 2 cm [1].
- A 2018 systematic review and meta-analysis of 5 RCTs and 14 cohort studies found no difference in functional outcome scores between surgical and nonsurgical management of type III injuries [4].
- In the nonsurgical group of type III injuries, patients had a faster return to work and sports but an inferior cosmetic appearance [4].
- A recent prospective randomized clinical trial found no statistical differences in validated outcome scores or return to preinjury sporting activity between surgical and nonsurgical management of acute type III and IV separations at 1 year follow-up [4].
- In a recent prospective randomized trial, the nonsurgical group had faster recovery than the surgical group for type III and IV separations [4].
- Five patients (16%) in the nonsurgical group of a recent trial required surgery for persistent symptoms at a mean of 8.7 months [4].
- A 2007 survey of 664 members and residency directors from the American Orthopaedic Society for Sports Medicine found that 86.3% preferred an initial trial of nonsurgical management for uncomplicated type III AC joint injuries [4].
- Surgical intervention for type III injuries is possible in the subacute or chronic setting if initial nonsurgical treatment fails [4].
- Early surgical repair of type III AC joint injuries with or without augmentation results in better patient satisfaction and clinical outcomes compared with delayed reconstruction [4].
- A 2016 systematic review found superior functional outcomes in the early surgical group compared with delayed surgery for complete AC joint dislocations involving mostly type III injuries [4].
- Partial dislocations or redislocations were found in 26% of cases in the early treatment group compared with 38.1% of cases in the delayed group [4].
- The rates of complication were 12.5% in the early surgical group and 17.7% in the delayed surgical group, though differences did not reach statistical significance [4].
- Surgery is indicated for most acute type IV, V, and VI separations [1].
- Nonsurgical treatment for type IV, V, and VI injuries likely results in substantial residual pain and limited function [1].
- Surgical indications for type III separations include younger, physically active patients, manual laborers, patients with cosmetic concerns, or those with chronic injuries who have persistent symptoms [1].
- Surgery is often recommended for patients with type IIIB (horizontally unstable) separations [1].
- Acute surgery (less than 3 to 4 weeks following injury) of high-grade AC joint separations can be successfully performed without the use of tendon graft if adequate reduction and stabilization are achieved [3].
- Delayed reconstruction of AC joint separations requires biologic augmentation, either ligament transfer or tendon grafting, in addition to CC stabilization [3].
- Anatomic AC joint reconstructions are biomechanically superior to nonanatomic techniques, such as the Weaver-Dunn procedure [3].
- Surgical indications for distal clavicle excision include persistent pain and failure of nonsurgical treatment in patients with AC joint arthritis [3].
- Relative contraindications for distal clavicle excision include a previous low-grade separation with persistent horizontal plane instability [3].
- Biomechanical evidence suggests a resection of 5 mm is needed to prevent contact between the clavicle and the acromion in the absence of instability [3].
- Care should be taken to preserve the posterior and superior AC ligaments during distal clavicle excision [3].
- Pain relief from distal clavicle excision is reliable in more than 90% of patients in the absence of instability [3].
- Previous traumatic instability is associated with persistent pain in 30% to 40% of cases following distal clavicle excision [3].
- One systematic review showed slightly better results with arthroscopic excision than with open distal clavicle excision [3].
- Direct comparison studies have shown similar or better results with arthroscopic excision than with open techniques [3].
- Between 5 and 10 mm of the distal clavicle should be resected in open distal clavicle resection (Mumford procedure) [3].
- Meticulous repair of the deltotrapezial fascia is important in open distal clavicle resection [3].
- Resection of the distal clavicle for AC joint arthritis should be limited to 5 to 10 mm of bone [3].
- Distal clavicle excision for the management of painful AC joint arthritis has a higher failure rate in patients with a history of previous low-grade AC joint separations [3].
- Postoperative care for AC joint reconstruction includes sling immobilization for 6 weeks to limit gravity forces on the operative construct [5].
- Hand, wrist, and elbow range of motion exercises, as well as pendulum exercises, are initiated immediately postoperatively following AC joint reconstruction [5].
- Physical therapy is begun at 4 weeks with gentle shoulder passive range of motion exercises following AC joint reconstruction [5].
- Unrestricted active motion is begun at 6 weeks following AC joint reconstruction [5].
- Strengthening exercises are initiated at 10 to 12 weeks following AC joint reconstruction [5].
- Subacute rehabilitation (1 to 6 weeks postoperative) involves gradually increasing shoulder range of motion, gentle passive stretching, and reducing sling use as pain permits [3].
- Late recovery rehabilitation (more than 6 weeks) involves full shoulder range of motion, stretching, and initiation of rotator cuff, scapular stabilizer, and deltoid strengthening [3].
- Heavy weight lifting and return to full activities are performed as tolerated during late recovery, with activity progression modified according to symptoms [3].
- Residual pain or soreness can persist for 3 to 4 months after distal clavicle excision and can be aggravated by heavy lifting [3].
- Complications associated with nonsurgical management of AC joint separations include persistent pain, crepitus, deformity, swelling at the AC joint, late arthrosis, and persistent instability [8].
- Osteolysis of the distal clavicle has been reported as a complication of nonsurgical management [8].
- Subacromial erosion can occur with the use of a hook plate [8].
- Implant failure and migration resulting in vascular or neurologic injuries have been reported with surgical management [8].
- Kirschner wires and pins are not advised for AC joint stabilization due to complications [8].
- Aseptic foreign body reaction and erosion of the coracoid or clavicle have been reported with the use of synthetic suture loops [8].
- Intrasubstance failure of synthetic grafts has been reported [8].
- Early or late fractures of the clavicle or coracoid process have been reported, especially with surgical techniques involving tunnels through the coracoid and/or clavicle [8].
- Painful implants related to the hook plate or CC screw usually require a second procedure for implant removal [8].
- Ossification of the CC space has been reported as a complication following surgery [8].
- Loss of AC joint reduction, persistent pain, and instability can potentially complicate surgical outcomes [8].
- Neurologic injuries are rare but can involve nerve root injuries secondary to traction, direct injury to the suprascapular nerve, or injury to the brachial plexus with techniques passing grafts or suture loops under the coracoid process [8].
- Adhesive capsulitis, osteomyelitis of the acromioclavicular joint, and upper extremity deep vein thrombosis have been reported as complications of AC joint surgery [8].
Complications¶
- AC joint separation is a common injury with an unknown incidence [1].
- Injury results in progressive disruption of the ligamentous support of the AC joint, beginning with the capsular ligaments and progressing to the CC ligaments [1].
- The mechanism of injury is usually direct trauma resulting from a fall on the point of the shoulder; indirect injuries are rare [1].
- Higher grade injuries result in prominence of the distal clavicle [1].
- Localized bruising, swelling, and tenderness are present in acute injuries [1].
- Range of motion and rotator cuff strength typically are normal in chronic injuries but may be limited in acute injuries secondary to pain [1].
- Scapular dyskinesis can be seen with AC joint injury [1].
- A coracoid fracture can result in superior displacement of the clavicle but an intact CC distance, creating a functionally equivalent AC joint separation [1].
- Weighted views help distinguish between type II and type III separations but rarely are indicated and often are not clinically helpful [1].
- Type III injuries are characterized by disruption of the AC and CC ligaments, increased CC distance, and superior displacement of the clavicle of up to 100% of the clavicle width [1].
- A modification of type III injuries has been proposed consisting of type IIIA (horizontally stable) and type IIIB (horizontally unstable) [1].
- Type IV injuries are characterized by disruption of the AC and CC ligaments with posterior displacement of the clavicle, increased CC distance, and the distal clavicle herniated into or through the deltotrapezial fascia [1].
- Type V injuries are characterized by disruption of the AC and CC ligaments with greater than 100% displacement of the clavicle superiorly, a markedly increased CC distance, and deformity usually not reducible because of herniation through the deltotrapezial fascia [1].
- Type VI injuries are characterized by disruption of the AC and CC ligaments with inferior clavicle displacement, resulting in the distal clavicle lying under the acromion or coracoid process [1].
- Patients with type I and II injuries treated nonsurgically are at increased risk for painful AC joint arthritis [1].
- Between 30% and 50% of young, very active patients will have mild to moderate residual pain at the AC joint after type I and II injuries [1].
- Meta-analysis and systematic reviews demonstrate similar outcomes for type III separations managed nonsurgically and surgically [1].
- Nonsurgical treatment for type III injuries resulted in quicker recovery and return to work compared to surgical treatment [1].
- Surgical treatment for type III injuries resulted in an increase in complications compared to nonsurgical treatment [1].
- One prospective, randomized trial showed better results with nonsurgical treatment when clavicle displacement was less than 2 cm and better results with surgical management when the clavicle was displaced more than 2 cm [1].
- Nonsurgical treatment for type IV, V, and VI injuries likely results in substantial residual pain and limited function [1].
- Patients are at risk for recurrent or persistent shoulder symptoms after type I and II injuries [4].
- Injury to the AC joint articular cartilage or articular disk can result in shoulder complaints subsequent to the injury [4].
- Retrospective studies have reported persistent symptoms in up to 40% to 50% of patients at 1, 6, and 10 years after type I and II injuries [4].
- In one study, 27% of patients underwent surgical intervention at a mean of 26 months after type I and II injuries [4].
- Distal clavicle resection can provide a potential solution in patients in whom nonsurgical treatment fails secondary to persistent AC joint inflammation or the development of osteoarthritis or distal clavicle osteolysis [4].
- A 2018 systematic review and meta-analysis found no difference between surgical and nonsurgical groups in terms of functional outcome scores for type III injuries [4].
- Patients in the nonsurgical group for type III injuries had a faster return to work and sports, although with an inferior cosmetic appearance [4].
- A recent prospective randomized clinical trial found no statistical differences in validated outcome scores or rates of return to preinjury sporting activity between surgical and nonsurgical groups for acute type III and IV injuries at 1 year follow-up [4].
- In a recent prospective randomized clinical trial, five patients (16%) in the nonsurgical group required surgery for persistent symptoms at a mean of 8.7 months [4].
- Early surgical repair of type III AC joint injuries with or without augmentation seems to result in better patient satisfaction and clinical outcomes compared with delayed reconstruction [4].
- A 2016 systematic review found superior functional outcomes in the early surgical group compared with delayed surgery for complete AC joint dislocation involving mostly type III injuries [4].
- Partial dislocations or redislocations were found in 26% of cases in the early treatment group compared with 38.1% of cases in the delayed group [4].
- The rates of complication were 12.5% in the early surgical group and 17.7% in the delayed surgical group, although the differences did not reach statistical significance [4].
- Surgical management is usually indicated for type IV and V AC joint separations given the high likelihood of persistent shoulder pain, dysfunction, and substantial deformity [4].
Key Evidence¶
References¶
[1] Aaos Comprehensive Orthopaedic Review 3. Disorders of the Acromioclavicular Joint > II. Traumatic Conditions of the AC Joint. [2] Orthopaedic Knowledge Update Sports Medicine 6. Disorders of the Acromioclavicular Joint, Sternoclavicular Joint, and Clavicle > AC Joint Injuries > Classification. [3] Aaos Comprehensive Orthopaedic Review 3. Disorders of the Acromioclavicular Joint > III. Atraumatic and Degenerative Conditions of the AC Joint. [4] Orthopaedic Knowledge Update Sports Medicine 6. Disorders of the Acromioclavicular Joint, Sternoclavicular Joint, and Clavicle > AC Joint Injuries > Management. [5] Campbell S Operative Orthopaedics 4 Volume Set. ARTHROSCOPIC REPAIR OF POSTERIOR HUMERAL AVULSION OF THE GLENOHUMERAL LIGAMENT > ARTHROSCOPICALLY ASSISTED AC JOINT RECONSTRUCTION > TECHNIQUE 52.28. [6] Orthopaedic Knowledge Update Sports Medicine 6. Disorders of the Acromioclavicular Joint, Sternoclavicular Joint, and Clavicle > AC Joint Injuries. [8] Orthopaedic Knowledge Update Sports Medicine 6. Disorders of the Acromioclavicular Joint, Sternoclavicular Joint, and Clavicle > AC Joint Injuries > Complications.