AC Joint Osteoarthritis PDF Evidence¶
AC joint osteoarthritis causes localized shoulder pain with cross-body movements; treatment ranges from activity modification to surgery.
What you're feeling¶
You likely feel pain at the very top of your shoulder, where your collarbone meets your shoulder blade. This is your acromioclavicular joint. The ache may stay mild for years. In fact, 90% of people with early signs on X-rays feel no pain at all over a 7-year period. However, if symptoms do start, they often follow a predictable pattern.
The pain usually worsens when you move your arm across your body. You might feel it when reaching up to a high shelf or behind your back to fasten a bra. Tucking in a shirt can also trigger a sharp pinch. Lifting objects, especially overhead, puts direct pressure on this joint. Many patients find that resting the arm at their side brings relief. Gentle movement often feels better than staying completely still.
Nighttime pain is a common complaint. You may wake up if you roll onto your affected shoulder. The weight of your body presses down on the inflamed joint, making it hard to find a comfortable position. Some people notice the pain is worse when they first wake up in the morning. It may feel stiff until you have moved around for a while.
It is important to know that imaging findings do not always match your symptoms. A distinction between symptomatic and asymptomatic radiographic AC osteoarthritis is unnecessary. All patients were equally satisfied with the outcome of preoperative acromioclavicular injection, regardless of what the X-rays showed. This means your level of discomfort is the true guide for treatment, not just the appearance of the joint on a scan.
If you have had previous shoulder surgery, such as a rotator cuff repair, untreated arthritis in this joint is associated with a low percentage of failure. It rarely causes major problems on its own. However, if you experience persistent pain that interferes with daily tasks like dressing or sleeping, your surgeon may discuss options like injections or minor surgery to remove the worn bone ends. These procedures provide predictable pain relief for symptomatic cases.
What's actually happening¶
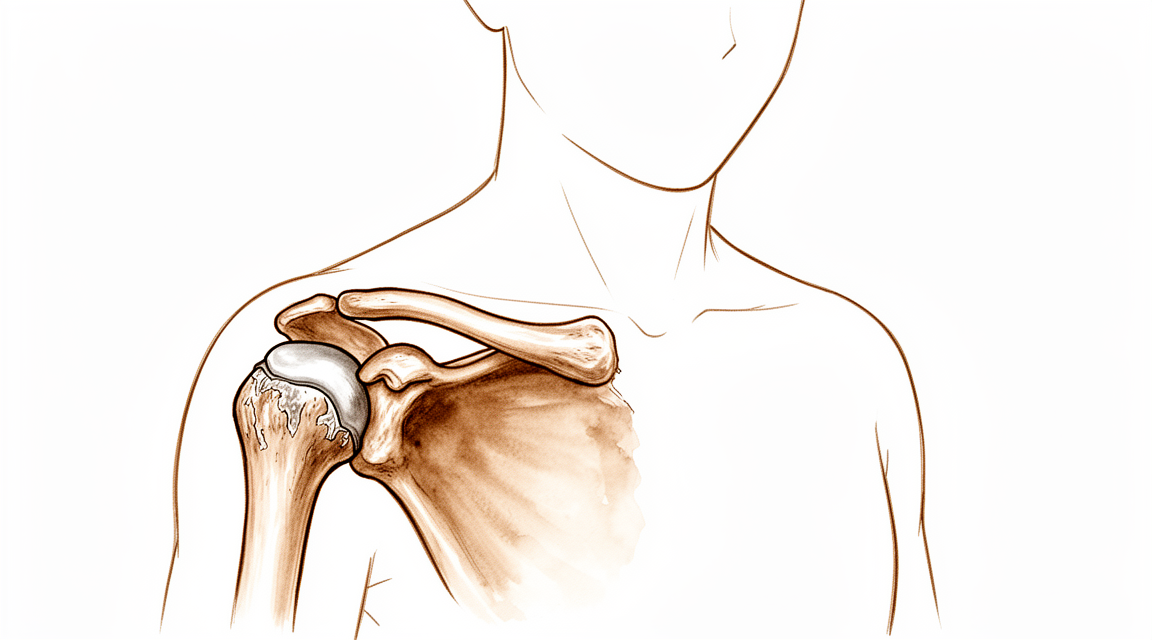
Your acromioclavicular (AC) joint sits at the very top of your shoulder, where your collarbone meets your shoulder blade. Think of this joint as a small hinge that allows your arm to move smoothly overhead. Inside, smooth cartilage acts like a shock absorber, cushioning the bones so they do not grind against each other.
In AC osteoarthritis, this protective cartilage wears down over time. It is essentially wear-and-tear arthritis. As the cushion thins, the bones rub together more directly. This friction causes inflammation and pain, especially when you reach across your body or lift your arm overhead. The joint capsule, which is the sleeve surrounding the joint, may also become stiff or irritated, adding to the discomfort.
Sometimes, the ligaments that hold your collarbone in place stretch or tear. This can cause the collarbone to sit higher than normal, creating a visible bump. When this happens, the normal movement of your shoulder blade changes. These kinematic changes can be a potential source of pain and dysfunction in the shoulder. Even if the joint looks fine on an X-ray, the altered movement can still cause symptoms.
It is important to know that not all changes on an X-ray mean you will have pain. Asymptomatic AC osteoarthritis remained asymptomatic in 90% of patients over a 7-year period. This means many people have visible wear on scans but feel no pain at all. Untreated AC joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure.
However, if the arthritis becomes severe, it can lead to other issues. Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty. Your surgeon will look at both your symptoms and your imaging to decide if the joint is truly the source of your pain.
The goal of treatment is to reduce this friction and restore smooth movement. Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis. These procedures involve removing a small part of the collarbone to create more space, allowing the bones to glide without rubbing. This simple change can significantly improve your shoulder function and reduce pain.
What we can do about it¶
You can start with self-management and physiotherapy. This conservative approach is a valid initial treatment for many shoulder injuries and joint conditions. Your surgeon may suggest modifying activities if you have osteolysis, which is the wearing away of bone. Physiotherapy aims to strengthen the muscles around your shoulder to support the joint. Conservative and surgical treatments are both effective for managing acromioclavicular joint osteoarthritis. Give this non-operative treatment a fair chance, as it is helpful for most patients with painful conditions in this area.
If pain persists, your surgeon may discuss medical management. This often includes pain medication and anti-inflammatory drugs to reduce swelling and discomfort. You might also consider acromioclavicular injections. These injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis. The injection helps reduce inflammation and pain directly at the joint site. Research is still comparing different types of steroid injections to see which works best for isolated joint pain. While some patients find lasting relief, others may need to explore other options if the injection effect wears off.
Surgery is considered when conservative care has reached its limit and pain continues to affect your daily life. Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic acromioclavicular osteoarthritis. This procedure involves removing a small part of the collarbone to create more space and reduce friction. Limited distal clavicle excision reduces pain and improves shoulder function at midterm follow-up in patients resistant to conservative treatment. Your surgeon will determine if you are a good candidate based on your specific symptoms and imaging results. For some, this simple removal of bone tissue is enough to restore comfort and movement without the need for more complex reconstruction.
What to expect¶
If you are diagnosed with wear-and-tear arthritis in the acromioclavicular (AC) joint but have no pain, it is likely to stay that way. In 90% of patients, asymptomatic AC osteoarthritis remained asymptomatic over a 7-year period. You do not need to worry about this finding if it is not bothering you. It is common to see signs of arthritis on scans even without symptoms.
If you have pain, the outlook depends on how you manage it. Injections into the joint offer a 1-year success rate of 47%. This means nearly half of patients find lasting relief from this treatment. If injections do not help, your surgeon may recommend a procedure to remove a small part of the collarbone. This limited distal clavicle excision reduces pain and improves shoulder function at midterm follow-up for patients who do not respond to conservative treatment.
You can expect predictable pain relief if you choose surgery. Both open and arthroscopic resection techniques provide this relief. However, each approach has a unique set of potential complications. Your surgeon will discuss which method is best for your specific anatomy and lifestyle.
If you leave symptomatic arthritis untreated, it may persist. Some patients experience ongoing discomfort that limits daily activities. If you undergo other shoulder surgeries, such as rotator cuff repair, untreated AC joint osteoarthritis is associated with a low percentage of failure. However, osteoarthritis is generally associated with poorer final clinical outcomes after rotator cuff repair. An unhealed or re-torn rotator cuff also increases the risk of developing this arthritis.
For severe cases, particularly if you are having a reverse shoulder replacement, severe AC joint osteoarthritis is associated with acromial stress fractures. Radiographic AC joint osteoarthritis is common in patients undergoing this type of surgery. Your surgeon will monitor these risks closely.
Overall, the course of AC joint arthritis varies. It can settle with conservative care, persist despite treatment, or progress slowly. Most patients find that targeted treatments provide significant improvement in function and comfort.
When to see someone¶
See your GP if you have persistent pain that does not improve with rest. Ask for a specialist review if you notice weakness or instability in the shoulder. Seek care if the joint locks or gives way. Contact your surgeon if symptoms interfere with your sleep or work. Sudden worsening of pain is also a reason to seek help. Note that asymptomatic wear-and-tear arthritis often remains painless for seven years. However, untreated issues can sometimes affect other shoulder repairs. Your doctor will check for tenderness and discuss if an injection might help. Early assessment ensures you get the right care before the condition progresses.
Evidence & references
title: "AC Joint Osteoarthritis" slug: ac-joint-osteoarthritis region: shoulder audience: patient mesh_terms: ["Acromioclavicular Joint", "Osteoarthritis", "Clavicle", "Joint Dislocations", "Ligaments, Articular", "Shoulder Pain", "Acromion", "Arthroplasty"] article_count: 271 model_used: Qwen3.6-35B-A3B-Q8_0.gguf generated_at: '2026-06-13T10:38:05+00:00' key_articles: - title: "Outcome of distal clavicle resection in patients with acromioclavicular joint osteoarthritis and full‐thickness rotator cuff tear" ref_num: 1 evidence_tier: paper evidence_level: 2 doi: 10.1007/s00167-014-3114-2 year: 2014 - title: "Seven-year course of asymptomatic acromioclavicular osteoarthritis diagnosed by MRI" ref_num: 2 evidence_tier: paper evidence_level: 2 doi: 10.1016/j.jse.2019.04.004 year: 2019 - title: "Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair" ref_num: 3 evidence_tier: paper evidence_level: 2 doi: 10.1007/s00167-020-06098-y year: 2020 - title: "The Role of Arthroscopy in Revision of Failed Open Anterior Stabilization of the Shoulder" ref_num: 4 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.arthro.2009.04.073 year: 2009 - title: "Factors Predicting the Outcome After Arthroscopically Assisted Stabilization of Acute High-Grade Acromioclavicular Joint Dislocations" ref_num: 5 evidence_tier: paper evidence_level: 3 doi: 10.1177/0363546519862850 year: 2019 - title: "Diagnostic value of a preoperative acromioclavicular injection for symptomatic acromioclavicular osteoarthritis: a retrospective study of cross-sectional midterm outcomes" ref_num: 6 evidence_tier: paper evidence_level: 4 doi: 10.5397/cise.2023.00073 year: 2024 - title: "Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty" ref_num: 7 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jseint.2021.11.008 year: 2022 - title: "Degenerative Joint Disease of the Acromioclavicular Joint" ref_num: 8 evidence_tier: paper evidence_level: 5 doi: 10.1177/0363546513485359 year: 2013 - title: "Limited distal clavicle excision of acromioclavicular joint osteoarthritis" ref_num: 9 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.otsr.2016.01.008 year: 2016 - title: "Editorial Commentary: Why We Have To Respect The Anatomy In Acromioclavicular Joint Surgery And Why Clinical Shoulder Scores Might Not Give Us The Information We Need!" ref_num: 10 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.arthro.2019.01.038 year: 2019 - title: "Improved identification of unstable acromioclavicular joint injuries in a clinical population using the acromial center line to dorsal clavicle radiographic measurement" ref_num: 12 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2019.12.014 year: 2020 - title: "Isolated acromioclavicular osteoarthritis and steroid injection" ref_num: 13 evidence_tier: paper evidence_level: 4 doi: 10.5397/cise.2023.00311 year: 2023 - title: "Arthroscopically assisted reduction of acute acromioclavicular joint dislocation using a single double-button device: Medium-term clinical and radiological outcomes" ref_num: 14 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.otsr.2017.11.001 year: 2018 - title: "Successful Conservative Therapy in Rockwood Type V Acromioclavicular Dislocations" ref_num: 15 evidence_tier: paper evidence_level: 4 doi: 10.1177/2325967115s00017 year: 2015 - title: "Instability and Degenerative Arthritis of the Sternoclavicular Joint" ref_num: 16 evidence_tier: paper evidence_level: 1 doi: 10.1177/0363546513498990 year: 2013 - title: "No differences between conservative and surgical management of acromioclavicular joint osteoarthritis: a scoping review" ref_num: 17 evidence_tier: paper evidence_level: 4 doi: 10.1007/s00167-020-06377-8 year: 2021 - title: "Preoperative Factors Associated With Subsequent Distal Clavicle Resection After Rotator Cuff Repair" ref_num: 18 evidence_tier: paper evidence_level: 3 doi: 10.1177/2325967119844295 year: 2019 - title: "Is Arthroscopic Distal Clavicle Resection Necessary for Patients With Radiological Acromioclavicular Joint Arthritis and Rotator Cuff Tears?" ref_num: 19 evidence_tier: paper evidence_level: 1 doi: 10.1177/0363546514547254 year: 2014 - title: "Arthroscopic versus open distal clavicle excision: Comparative results at six months and one year from a randomized, prospective clinical trial" ref_num: 20 evidence_tier: paper evidence_level: 1 doi: 10.1016/j.jse.2006.10.006 year: 2007 - title: "Surgical treatment of chronic acromioclavicular dislocation: Comparison between two surgical procedures for anatomic reconstruction" ref_num: 21 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.injury.2010.09.023 year: 2010 - title: "Mid- to long-term success rate and functional outcomes of acromioclavicular injections in patients with acromioclavicular osteoarthritis" ref_num: 22 evidence_tier: paper evidence_level: 4 doi: 10.5397/cise.2023.00031 year: 2023 - title: "Osteoarthritis after rotator cuff repair: A 10-year follow-up study" ref_num: 23 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.otsr.2017.03.007 year: 2017 - title: "The ligamentous injury pattern in acute acromioclavicular dislocations and its impact on clinical and radiographic parameters" ref_num: 24 evidence_tier: paper evidence_level: 1 doi: 10.1016/j.jse.2020.10.026 year: 2021 - title: "Acute grade III and IV acromioclavicular dislocations: Outcomes and pitfalls of reconstruction procedures using a synthetic ligament" ref_num: 25 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.otsr.2010.06.004 year: 2010 - title: "Differences between Coracoclavicular, Acromioclavicular, or Combined Reconstruction Techniques on the Kinematics of the Shoulder Girdle" ref_num: 26 evidence_tier: paper evidence_level: 5 doi: 10.1177/03635465221095231 year: 2022 - title: "The Function of the Acromioclavicular and Coracoclavicular Ligaments in Shoulder Motion" ref_num: 27 evidence_tier: paper evidence_level: 5 doi: 10.1177/0363546512458571 year: 2012 - title: "Acromioclavicular joint ligamentous system contributing to clavicular strut function: a cadaveric study" ref_num: 28 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jse.2013.01.004 year: 2013 - title: "Subacromial morphometric assessment of the clavicle hook plate" ref_num: 29 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.injury.2009.12.012 year: 2010 - title: "Can an acute high-grade acromioclavicular joint separation be reduced and stabilized without surgery? A surgeon’s experience" ref_num: 33 evidence_tier: paper evidence_level: 4 doi: 10.1007/s00402-020-03630-0 year: 2020 - title: "Current concepts in acromioclavicular joint (AC) instability – a proposed treatment algorithm for acute and chronic AC-joint surgery" ref_num: 35 evidence_tier: paper evidence_level: 5 doi: 10.1186/s12891-022-05935-0 year: 2022 - title: "Current Concepts in the Operative Management of Acromioclavicular Dislocations: A Systematic Review and Meta-analysis of Operative Techniques" ref_num: 38 evidence_tier: paper evidence_level: 1 doi: 10.1177/0363546518795147 year: 2018 - title: "Arthroscopic Coracoclavicular Ligament Reconstruction With Double‐Bundle Soft Tissue Allograft for Chronic Type V Acromioclavicular Dislocations Shows Excellent Patient Outcomes and Return to Duty and Sport at Minimum 10‐Year Follow‐Up" ref_num: 39 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.arthro.2025.05.008 year: 2025 - title: "Acromioclavicular joint augmentation at the time of coracoclavicular ligament reconstruction fails to improve functional outcomes despite significantly improved horizontal stability" ref_num: 41 evidence_tier: paper evidence_level: 1 doi: 10.1007/s00167-018-5152-7 year: 2018 - title: "Histologic and magnetic resonance image evaluation in acromioclavicular joint osteoarthritis" ref_num: 43 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jseint.2020.03.007 year: 2020 - title: "Painful Conditions of the Acromioclavicular Joint" ref_num: 44 evidence_tier: paper evidence_level: 5 doi: 10.5435/00124635-199905000-00004 year: 1999 - title: "Additional acromioclavicular cerclage limits lateral tilt of the scapula in patients with arthroscopically assisted coracoclavicular ligament reconstruction" ref_num: 45 evidence_tier: paper evidence_level: 3 doi: 10.1007/s00402-021-03761-y year: 2021 - title: "Minimally Invasive Coracoclavicular Ligament Augmentation With a Flip Button/Polydioxanone Repair for Treatment of Total Acromioclavicular Joint Dislocation" ref_num: 48 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.arthro.2006.12.015 year: 2007 - title: "Conversion to anatomic coracoclavicular ligament reconstruction (ACCR) shows similar clinical outcomes compared to successful non‐operative treatment in chronic primary type III to V acromioclavicular joint injuries" ref_num: 49 evidence_tier: paper evidence_level: 4 doi: 10.1007/s00167-020-06159-2 year: 2020 - title: "Complication rates and types of failure after arthroscopic acute acromioclavicular dislocation fixation. Prospective multicenter study of 116 cases" ref_num: 50 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.otsr.2015.09.012 year: 2015 synthesis_version: "v2" verifier_status: skipped
Overview¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis [8].
- Open and arthroscopic resection arthroplasty techniques have unique sets of potential complications that may be minimized with improved understanding of anatomy, biomechanics, and meticulous surgical technique [8].
- Limited distal clavicle excision reduced pain and improved shoulder function at midterm follow-up in patients with AC joint osteoarthritis resistant to conservative treatment [9].
- A distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Further characterisation of patients in whom mild arthroscopic findings of OA of the AC joint are clinically significant and warrant resection is needed [1].
- Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair [3].
- Clinicians should consider overreduction of the AC joint because it may lead to favorable radiological results [5].
- The authors recommend anatomic reconstruction procedures for the treatment of chronic complete AC dislocations [21].
Anatomy & Pathophysiology¶
- Anatomic techniques that address both coracoclavicular ligaments and the AC capsule are recommended to restore horizontal and vertical stability while allowing physiological rotation [10].
- None of the reconstruction strategies completely restored the shoulder girdle to its preinjured state [26].
- Kinematic changes resulting from AC joint dislocation could be a potential source of pain and dysfunction in the shoulder [27].
- Scapular and clavicular kinematics were affected in AC separation models [28].
- The position of the hook portion of a clavicle hook plate can predispose anatomic structures to post-operative complications of subacromial impingement and bony erosion [29].
- Future research should focus on addressing horizontal and rotational instability to restore native physiological and biomechanical properties of the AC joint [35].
- Coracoclavicular reconstruction with augmentation of the acromioclavicular joint provides improved horizontal stability compared to isolated coracoclavicular reconstruction [41].
- Adding a fixation of the AC joint minimizes lateral tilting of the scapula and maintains a more anatomic reposition result over time [45].
Classification¶
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Mild arthroscopic findings of acromioclavicular joint osteoarthritis may be clinically significant and warrant resection, but further characterization of such patients is needed [1].
- Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Radiographic acromioclavicular joint osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Osteolytic changes in the acromioclavicular joint seemed to be associated with incongruity of the joint but did not correlate with clinical results [11].
- The acromial center line to dorsal clavicle radiographic measurement and the use of the Alexander view provide a more realistic appreciation of true acromioclavicular joint displacement, especially in defining watershed cases (Rockwood types IIIA, IIB, and IV) [12].
- Evaluating the integrity of the capsuloligamentous structures stabilizing the acromioclavicular joint is reproducible and provides additional information on the severity of the injury [24].
- Injuries to the sternoclavicular joint are uncommon, and recognition and classification are critical to proper management to minimize long-term sequelae [16].
- Some persistent pain and osteoarthritis progression remain concerns in the arthroscopic revision of failed open anterior stabilization of the shoulder [4].
Clinical Presentation¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Preventive arthroscopic distal clavicle resection is not recommended in patients with radiological but asymptomatic ACJ arthritis [19].
- Further characterisation of patients in whom mild arthroscopic findings of OA of the AC joint are clinically significant and warrant resection is needed [1].
- A distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Osteolytic changes seemed to be associated with incongruity of the AC joint, but did not correlate with clinical results [11].
- Additional research is needed to determine the main cause of pain in isolated acromioclavicular osteoarthritis and to compare clinical outcomes of intra-articular versus extra-articular injections [13].
- Risk factors for subsequent distal clavicle excision after rotator cuff repair include tenderness to palpation at the AC joint, female sex, and surgery on the dominant side [18].
- Subsequent distal clavicle excision was performed in 40% of cases with a combination of the three identified risk factors (tenderness to palpation, female sex, dominant side surgery) [18].
- Recurrence of the initial dislocation after arthroscopically assisted reduction appears to be related to the onset of degenerative ACJ arthropathy [14].
- Some persistent pain and osteoarthritis progression remain concerns in the revision of failed open anterior stabilization of the shoulder [4].
Investigations¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Preventive arthroscopic distal clavicle resection (DCR) is not recommended in patients with radiological but asymptomatic ACJ arthritis [19].
- Further characterization is needed to determine which patients with mild arthroscopic findings of AC joint OA are clinically significant and warrant resection [1].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty (RSA) [7].
- Severe ACJ osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Osteolytic changes in the AC joint seemed to be associated with incongruity but did not correlate with clinical results [11].
- Patients with edema on MRI were more likely to present with pain than patients without edema [43].
- Subchondral bone edema on histologic examination was more frequent in patients with pain [43].
- The outcomes of a preoperative AC injection suggest that a distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome [6].
- Additional research is needed to determine the main cause of pain and to compare clinical outcomes of intra-articular versus extra-articular steroid injections for isolated AC osteoarthritis [13].
- Risk factors for subsequent distal clavicle excision after rotator cuff repair include tenderness to palpation at the AC joint, female sex, and surgery on the dominant side [18].
- Subsequent distal clavicle excision was performed in 40% of cases with a combination of the three identified risk factors (tenderness, female sex, dominant side) [18].
- The arthroscopic approach offers an advantage in diagnosing and treating occult intra-articular pathology during distal clavicle excision [20].
- Some persistent pain and osteoarthritis progression remain concerns in the revision of failed open anterior stabilization of the shoulder using arthroscopy [4].
- Evaluating the integrity of the capsuloligamentous structures stabilizing the AC joint is reproducible and provides additional information on injury severity, which may influence treatment decisions [24].
- The AC-DC measurement and use of the Alexander view provide a more realistic appreciation of true AC joint displacement, particularly in defining watershed cases (IIIA/IIB/IV) [12].
- Radiological failures were observed in 41% of cases in a prospective multicenter study of arthroscopic acute AC dislocation fixation [50].
Treatment¶
Non-Operative Management¶
- Conservative therapy is a valid initial treatment option for Rockwood Type V acromioclavicular dislocations [15].
- Non-operative reduction and stabilization is a valuable treatment option for acute high-grade acromioclavicular joint separations [33].
- Nonoperative treatment is helpful for most patients with painful conditions of the acromioclavicular joint, although those with osteolysis may need to modify their activities [44].
- Conservative and surgical treatments are both effective in the management of acromioclavicular joint osteoarthritis [17].
- Acromioclavicular injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis [22].
- Additional research is needed to determine the main cause of pain and to compare clinical outcomes of intra-articular versus extra-articular steroid injections for isolated acromioclavicular osteoarthritis [13].
Operative Management¶
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic acromioclavicular osteoarthritis [8].
- Limited distal clavicle excision reduces pain and improves shoulder function at midterm follow-up in patients with acromioclavicular joint osteoarthritis resistant to conservative treatment [9].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Further characterization is needed to identify patients in whom mild arthroscopic findings of acromioclavicular joint osteoarthritis are clinically significant and warrant resection [1].
- Conversion to anatomic coracoclavicular ligament reconstruction shows similar clinical outcomes compared to successful non-operative treatment in chronic primary type III to V acromioclavicular joint injuries at a minimum 5-year follow-up [49].
- The authors recommend anatomic reconstruction procedures for the treatment of chronic complete acromioclavicular dislocations [21].
- Osteoarthritis is associated with poorer final clinical outcomes after rotator cuff repair, and an unhealed or re-torn cuff increases the risk of osteoarthritis [23].
Diagnostic Considerations¶
- A distinction between symptomatic and asymptomatic radiographic acromioclavicular osteoarthritis appears unnecessary, as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year course [2].
- Some persistent pain and osteoarthritis progression remain concerns following arthroscopy in the revision of failed open anterior stabilization of the shoulder [4].
Complications¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Osteoarthritis is associated with poorer final clinical outcomes after rotator cuff repair [23].
- An unhealed or re-torn rotator cuff increases the risk of developing osteoarthritis [23].
- Severe AC joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Some persistent pain and osteoarthritis progression remain concerns following arthroscopy in revision of failed open anterior stabilization of the shoulder [4].
- Recurrence of the initial dislocation after arthroscopically assisted reduction of acute AC joint dislocation appears to be related to the onset of degenerative ACJ arthropathy [14].
- Treatment of acute grade III and IV AC dislocations by synthetic ligament reconstruction carries a risk of significant early osteolysis [25].
- Open and arthroscopic AC joint reconstruction techniques have no differences in loss of reduction, complication rate, or revision rate [38].
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis but each has a unique set of potential complications [8].
Recovery¶
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Limited distal clavicle excision for acromioclavicular joint osteoarthritis resistant to conservative treatment reduced pain and improved shoulder function at midterm follow-up [9].
- Acromioclavicular injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis [22].
- A preoperative acromioclavicular injection study suggested that distinguishing between symptomatic and asymptomatic radiographic acromioclavicular osteoarthritis is unnecessary, as all patients were equally satisfied with the outcome [6].
- Osteolytic changes in the acromioclavicular joint seemed to be associated with incongruity but did not correlate with clinical results [11].
- Recurrence of initial acromioclavicular joint dislocation appears to be related to the onset of degenerative acromioclavicular joint arthropathy [14].
- Treatment of acute grade III and IV acromioclavicular dislocations using synthetic ligament reconstruction gave satisfactory results in terms of recovery of strength, but evolution is not risk-free due to the onset of significant early osteolysis [25].
- Arthroscopic coracoclavicular ligament reconstruction with double-bundle soft tissue allograft for chronic type V acromioclavicular dislocations showed sustained and statistically significant improvements in functional outcomes, high rates of return to sport, and maintenance of active-duty military status at minimum 10-year follow-up [39].
- Minimally invasive coracoclavicular ligament augmentation with a flip button/polydioxanone repair for total acromioclavicular joint dislocation revealed excellent radiologic and clinical results with no subluxations or dislocations noted in short-term follow-up [48].
- Some persistent pain and osteoarthritis progression remain concerns in the arthroscopic revision of failed open anterior stabilization of the shoulder [4].
- Type V acromioclavicular dislocations may be given a trial of conservative therapy [15].
Key Evidence¶
- [L2] Further characterisation of patients in whom mild arthroscopic findings of OA of AC joint are clinically significant and warrant resection is needed. (10.1007/s00167-014-3114-2)
- [L2] Asymptomatic AC-OA remained asymptomatic in 90% over 7 years. (10.1016/j.jse.2019.04.004)
- [L2] Untreated ACJ osteoarthritis, symptomatic or not, encountered during arthroscopic RCR is associated with a low percentage of failure. (10.1007/s00167-020-06098-y)
- [L4] Some persistent pain and osteoarthritis progression remain concerns. (10.1016/j.arthro.2009.04.073)
- [L3] Clinicians should consider overreduction of the AC joint because it may lead to favorable radiological results. (10.1177/0363546519862850)
- [L4] The outcomes of this study seem to suggest that a distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome. (10.5397/cise.2023.00073)
- [L3] Radiographic ACJ osteoarthritis is common in patients undergoing RSA. (10.1016/j.jseint.2021.11.008)
- [L5] Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis, though each has a unique set of potential complications that may be minimized with improved understanding of anatomy, biomechanics, and meticulous surgical technique. (10.1177/0363546513485359)
- [L4] Limited distal clavicle excision of patients with AC joint osteoarthritis resistant to conservative treatment reduced pain and improved shoulder function at midterm follow-up. (10.1016/j.otsr.2016.01.008)
- [L5] Anatomic techniques that address both coracoclavicular ligaments and the AC capsule are recommended to restore horizontal and vertical stability while allowing physiological rotation. (10.1016/j.arthro.2019.01.038)
- [L4] The AC-DC measurement and use of the Alexander view provides the clinician with a more realistic appreciation of true AC joint displacement, especially in defining watershed cases (ie, IIIA/IIB/IV) and may better inform the decision-making process regarding management options and recommendations. (10.1016/j.jse.2019.12.014)
- [L4] Additional research is needed to determine the main cause of pain and compare clinical outcomes of intra-articular versus extra-articular injections. (10.5397/cise.2023.00311)
- [L4] Recurrence of the initial dislocation appears to be related to onset of degenerative ACJ arthropathy. (10.1016/j.otsr.2017.11.001)
- [L4] This suggests that Type V AC dislocations may be given a trial of conservative therapy. (10.1177/2325967115s00017)
- [L1] Injuries to the SC joint are uncommon, and recognition and classification are critical to proper management to minimize long-term sequelae. (10.1177/0363546513498990)
- [L4] Conservative and surgical treatments are both effective in acromioclavicular joint osteoarthritis management. (10.1007/s00167-020-06377-8)
- [L3] Risk factors for subsequent DCE included tenderness to palpation at the AC joint, female sex, and surgery on the dominant side, with subsequent DCE performed in 40% of cases with a combination of these 3 factors. (10.1177/2325967119844295)
- [L1] Preventive arthroscopic DCR is not recommended in patients with radiological but asymptomatic ACJ arthritis. (10.1177/0363546514547254)
- [L1] The arthroscopic approach offers a unique advantage in diagnosing and treating occult intra-articular pathology. (10.1016/j.jse.2006.10.006)
- [L4] The authors recommend this procedure for the treatment of chronic complete AC dislocations. (10.1016/j.injury.2010.09.023)
- [L4] AC injections offer a 1-year success rate of 47%. (10.5397/cise.2023.00031)
- [L4] Osteoarthritis is associated with poorer final clinical outcomes, and an unhealed or re-torn cuff increases the risk of osteoarthritis. (10.1016/j.otsr.2017.03.007)
- [L1] Evaluating the integrity of the capsuloligamentous structures stabilizing the AC joint is reproducible and gives additional information on the severity of the injury, which might also influence the treatment decision. (10.1016/j.jse.2020.10.026)
- [L4] Treatment of ACD by synthetic ligament reconstruction gave satisfactory results, notably in terms of recovery of strength, but evolution is not risk-free with onset of significant early osteolysis. (10.1016/j.otsr.2010.06.004)
- [L5] Although each technique was able to restore different elements of the joint kinematics, none of the strategies completely restored the shoulder girdle to its preinjured state. (10.1177/03635465221095231)
- [L5] The kinematic changes could be a potential source of pain and dysfunction in the shoulder with AC joint dislocation. (10.1177/0363546512458571)
- [L5] Scapular and clavicular kinematics were affected in AC separation models. (10.1016/j.jse.2013.01.004)
- [L5] The observed frequency of hook contact with surrounding subacromial structures in a static shoulder confirms that the position of the hook portion of the implant can predispose anatomic structures to the post-operative complications of subacromial impingement and bony erosion. (10.1016/j.injury.2009.12.012)
- [L4] Non-operative reduction and stabilization of high-grade AC joint separations seems to be a valuable treatment option. (10.1007/s00402-020-03630-0)
- [L5] Future research should focus on addressing horizontal and rotational instability, to restore native physiological and biomechanical properties of the AC joint. (10.1186/s12891-022-05935-0)
- [L1] Open and arthroscopic AC joint reconstruction techniques have no differences in loss of reduction, the complication rate, and the revision rate based on the available literature. (10.1177/0363546518795147)
- [L4] Outcomes after arthroscopic CC reconstruction for chronic, type V AC dislocations in an active-duty military patient population show sustained and statistically significant improvements in functional outcomes as well as high rates of return to sport and maintenance of active-duty military status at long-term follow-up. (10.1016/j.arthro.2025.05.008)
- [L1] Coracoclavicular reconstruction with augmentation of the acromioclavicular joint has been shown to provide improved horizontal stability in both biomechanical and clinical studies compared to isolated coracoclavicular reconstruction. (10.1007/s00167-018-5152-7)
- [L4] Patients with edema on MRI were more likely to present pain than patients without edema, and subchondral bone edema on histologic examination was more frequent in patients with pain. (10.1016/j.jseint.2020.03.007)
- [L5] Nonoperative treatment is helpful for most patients, although those with osteolysis may have to modify their activities. (10.5435/00124635-199905000-00004)
- [L3] The presented data suggest adding a fixation of the AC joint to minimize lateral tilting of the scapula and maintain a more anatomic reposition result over time. (10.1007/s00402-021-03761-y)
- [L4] The short-term follow-up of 15 recently operated patients reveals excellent radiologic and clinical results, with no subluxations or dislocations of the acromioclavicular joint noted. (10.1016/j.arthro.2006.12.015)
- [L4] At a minimum 5-year follow-up, patients with successful non-operative treatment for type III-V ACJ injuries achieved similar clinical outcomes compared to those who were converted to ACCR. (10.1007/s00167-020-06159-2)
- [L4] Surgery for AC dislocations is difficult with radiological results that must still be improved, as radiological failures were observed in 41% of cases. (10.1016/j.otsr.2015.09.012)
References¶
[1] Outcome of distal clavicle resection in patients with acromioclavicular joint osteoarthritis and full‐thickness rotator cuff tear. Knee Surgery, Sports Traumatology, Arthroscopy. 2014. DOI: 10.1007/s00167-014-3114-2 [2] Seven-year course of asymptomatic acromioclavicular osteoarthritis diagnosed by MRI. Journal of Shoulder and Elbow Surgery. 2019. DOI: 10.1016/j.jse.2019.04.004 [3] Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair. Knee Surgery, Sports Traumatology, Arthroscopy. 2020. DOI: 10.1007/s00167-020-06098-y [4] The Role of Arthroscopy in Revision of Failed Open Anterior Stabilization of the Shoulder. Arthroscopy. 2009. DOI: 10.1016/j.arthro.2009.04.073 [5] Factors Predicting the Outcome After Arthroscopically Assisted Stabilization of Acute High-Grade Acromioclavicular Joint Dislocations. The American Journal of Sports Medicine. 2019. DOI: 10.1177/0363546519862850 [6] Diagnostic value of a preoperative acromioclavicular injection for symptomatic acromioclavicular osteoarthritis: a retrospective study of cross-sectional midterm outcomes. Clinics in Shoulder and Elbow. 2024. DOI: 10.5397/cise.2023.00073 [7] Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty. JSES International. 2022. DOI: 10.1016/j.jseint.2021.11.008 [8] Degenerative Joint Disease of the Acromioclavicular Joint. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513485359 [9] Limited distal clavicle excision of acromioclavicular joint osteoarthritis. Orthopaedics & Traumatology: Surgery & Research. 2016. DOI: 10.1016/j.otsr.2016.01.008 [10] Editorial Commentary: Why We Have To Respect The Anatomy In Acromioclavicular Joint Surgery And Why Clinical Shoulder Scores Might Not Give Us The Information We Need!. Arthroscopy. 2019. DOI: 10.1016/j.arthro.2019.01.038 [11] 10.1016-0020-1383-83-90092-x. n.d.. [12] Improved identification of unstable acromioclavicular joint injuries in a clinical population using the acromial center line to dorsal clavicle radiographic measurement. Journal of Shoulder and Elbow Surgery. 2020. DOI: 10.1016/j.jse.2019.12.014 [13] Isolated acromioclavicular osteoarthritis and steroid injection. Clinics in Shoulder and Elbow. 2023. DOI: 10.5397/cise.2023.00311 [14] Arthroscopically assisted reduction of acute acromioclavicular joint dislocation using a single double-button device: Medium-term clinical and radiological outcomes. Orthopaedics & Traumatology: Surgery & Research. 2018. DOI: 10.1016/j.otsr.2017.11.001 [15] Successful Conservative Therapy in Rockwood Type V Acromioclavicular Dislocations. Orthopaedic Journal of Sports Medicine. 2015. DOI: 10.1177/2325967115s00017 [16] Instability and Degenerative Arthritis of the Sternoclavicular Joint. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513498990 [17] No differences between conservative and surgical management of acromioclavicular joint osteoarthritis: a scoping review. Knee Surgery, Sports Traumatology, Arthroscopy. 2021. DOI: 10.1007/s00167-020-06377-8 [18] Preoperative Factors Associated With Subsequent Distal Clavicle Resection After Rotator Cuff Repair. Orthopaedic Journal of Sports Medicine. 2019. DOI: 10.1177/2325967119844295 [19] Is Arthroscopic Distal Clavicle Resection Necessary for Patients With Radiological Acromioclavicular Joint Arthritis and Rotator Cuff Tears?. The American Journal of Sports Medicine. 2014. DOI: 10.1177/0363546514547254 [20] Arthroscopic versus open distal clavicle excision: Comparative results at six months and one year from a randomized, prospective clinical trial. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.10.006 [21] Surgical treatment of chronic acromioclavicular dislocation: Comparison between two surgical procedures for anatomic reconstruction. Injury. 2010. DOI: 10.1016/j.injury.2010.09.023 [22] Mid- to long-term success rate and functional outcomes of acromioclavicular injections in patients with acromioclavicular osteoarthritis. Clinics in Shoulder and Elbow. 2023. DOI: 10.5397/cise.2023.00031 [23] Osteoarthritis after rotator cuff repair: A 10-year follow-up study. Orthopaedics & Traumatology: Surgery & Research. 2017. DOI: 10.1016/j.otsr.2017.03.007 [24] The ligamentous injury pattern in acute acromioclavicular dislocations and its impact on clinical and radiographic parameters. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2020.10.026 [25] Acute grade III and IV acromioclavicular dislocations: Outcomes and pitfalls of reconstruction procedures using a synthetic ligament. Orthopaedics & Traumatology: Surgery & Research. 2010. DOI: 10.1016/j.otsr.2010.06.004 [26] Differences between Coracoclavicular, Acromioclavicular, or Combined Reconstruction Techniques on the Kinematics of the Shoulder Girdle. The American Journal of Sports Medicine. 2022. DOI: 10.1177/03635465221095231 [27] The Function of the Acromioclavicular and Coracoclavicular Ligaments in Shoulder Motion. The American Journal of Sports Medicine. 2012. DOI: 10.1177/0363546512458571 [28] Acromioclavicular joint ligamentous system contributing to clavicular strut function: a cadaveric study. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2013.01.004 [29] Subacromial morphometric assessment of the clavicle hook plate. Injury. 2010. DOI: 10.1016/j.injury.2009.12.012 [33] Can an acute high-grade acromioclavicular joint separation be reduced and stabilized without surgery? A surgeon’s experience. Archives of Orthopaedic and Trauma Surgery. 2020. DOI: 10.1007/s00402-020-03630-0 [35] Current concepts in acromioclavicular joint (AC) instability – a proposed treatment algorithm for acute and chronic AC-joint surgery. BMC Musculoskeletal Disorders. 2022. DOI: 10.1186/s12891-022-05935-0 [38] Current Concepts in the Operative Management of Acromioclavicular Dislocations: A Systematic Review and Meta-analysis of Operative Techniques. The American Journal of Sports Medicine. 2018. DOI: 10.1177/0363546518795147 [39] Arthroscopic Coracoclavicular Ligament Reconstruction With Double‐Bundle Soft Tissue Allograft for Chronic Type V Acromioclavicular Dislocations Shows Excellent Patient Outcomes and Return to Duty and Sport at Minimum 10‐Year Follow‐Up. Arthroscopy. 2025. DOI: 10.1016/j.arthro.2025.05.008 [41] Acromioclavicular joint augmentation at the time of coracoclavicular ligament reconstruction fails to improve functional outcomes despite significantly improved horizontal stability. Knee Surgery, Sports Traumatology, Arthroscopy. 2018. DOI: 10.1007/s00167-018-5152-7 [43] Histologic and magnetic resonance image evaluation in acromioclavicular joint osteoarthritis. JSES International. 2020. DOI: 10.1016/j.jseint.2020.03.007 [44] Painful Conditions of the Acromioclavicular Joint. Journal of the American Academy of Orthopaedic Surgeons. 1999. DOI: 10.5435/00124635-199905000-00004 [45] Additional acromioclavicular cerclage limits lateral tilt of the scapula in patients with arthroscopically assisted coracoclavicular ligament reconstruction. Archives of Orthopaedic and Trauma Surgery. 2021. DOI: 10.1007/s00402-021-03761-y [48] Minimally Invasive Coracoclavicular Ligament Augmentation With a Flip Button/Polydioxanone Repair for Treatment of Total Acromioclavicular Joint Dislocation. Arthroscopy. 2007. DOI: 10.1016/j.arthro.2006.12.015 [49] Conversion to anatomic coracoclavicular ligament reconstruction (ACCR) shows similar clinical outcomes compared to successful non‐operative treatment in chronic primary type III to V acromioclavicular joint injuries. Knee Surgery, Sports Traumatology, Arthroscopy. 2020. DOI: 10.1007/s00167-020-06159-2 [50] Complication rates and types of failure after arthroscopic acute acromioclavicular dislocation fixation. Prospective multicenter study of 116 cases. Orthopaedics & Traumatology: Surgery & Research. 2015. DOI: 10.1016/j.otsr.2015.09.012