DRUJ Hemiresection Arthroplasty PDF Evidence¶
A recovery plan after hemiresection-interposition arthroplasty of the distal radioulnar joint, where the worn part of the ulnar head is partially removed to restore pain-free forearm rotation; after a brief period of protection, early forearm rotation (turning the palm up and down) is the priority, with heavier loading added gradually.
This protocol guides your recovery after hemiresection-interposition arthroplasty of the distal radioulnar joint (DRUJ) — an operation that reshapes the worn end of the forearm to restore comfortable, pain-free rotation of the forearm — with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist — bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
The distal radioulnar joint (DRUJ) is the small joint near your wrist on the little-finger side where the two forearm bones — the radius and the ulna — meet. It is the joint that lets you turn your forearm over, palm up (supination) and palm down (pronation). When this joint wears out and becomes arthritic, turning the forearm becomes painful.
In a hemiresection arthroplasty, only the worn, arthritic part of the head of the ulna is shaved away (a partial removal — "hemi" means half), and a small cushion of your own soft tissue is tucked into the gap to keep the surfaces from rubbing. Importantly, this operation preserves the key stabilising structures — the TFCC (the cartilage and ligament hammock that supports the wrist on that side), the ulnar styloid, and the soft-tissue attachments — so the end of the ulna stays supported. This is what makes it different from a complete removal of the ulnar head (a Darrach procedure).
Because the joint surfaces are reshaped rather than repaired or reconstructed, there is no tendon or ligament that has to heal under protection for months. The single goal of this operation is pain-free forearm rotation, and so the single most important part of your rehabilitation is getting that rotation moving early. After a brief period of protection in a splint to let the soft tissues settle, restoring the turn of the forearm — palm up and palm down — becomes the headline of your recovery. Strength and heavier loading are added gradually afterwards.
Precautions and limitations¶
- For about the first two to three weeks, wear your splint as directed — it gently limits forearm rotation while the interposition tissue settles. Keep your fingers, and (when allowed) your wrist, moving throughout.
- Once cleared out of the splint, make gentle forearm rotation your priority — but keep it pain-free and unloaded. Early rotation should be done with an empty hand, not against weight.
- Do NOT load the forearm in rotation early — no twisting open jars, wringing cloths, using a screwdriver, or carrying heavy bags on that side until strengthening is cleared (commonly around six to eight weeks).
- Be alert to pain or a sense of instability on the little-finger side of the wrist when you push or load through the forearm — this is the area the operation works on. Mention it to your hand therapist; do not push through it.
- Keep your fingers, thumb, elbow and shoulder moving freely from the start, and use the hand for light everyday tasks within comfort, as long as it does not involve forced or loaded twisting.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises¶
Kieran Hirpara 4.0
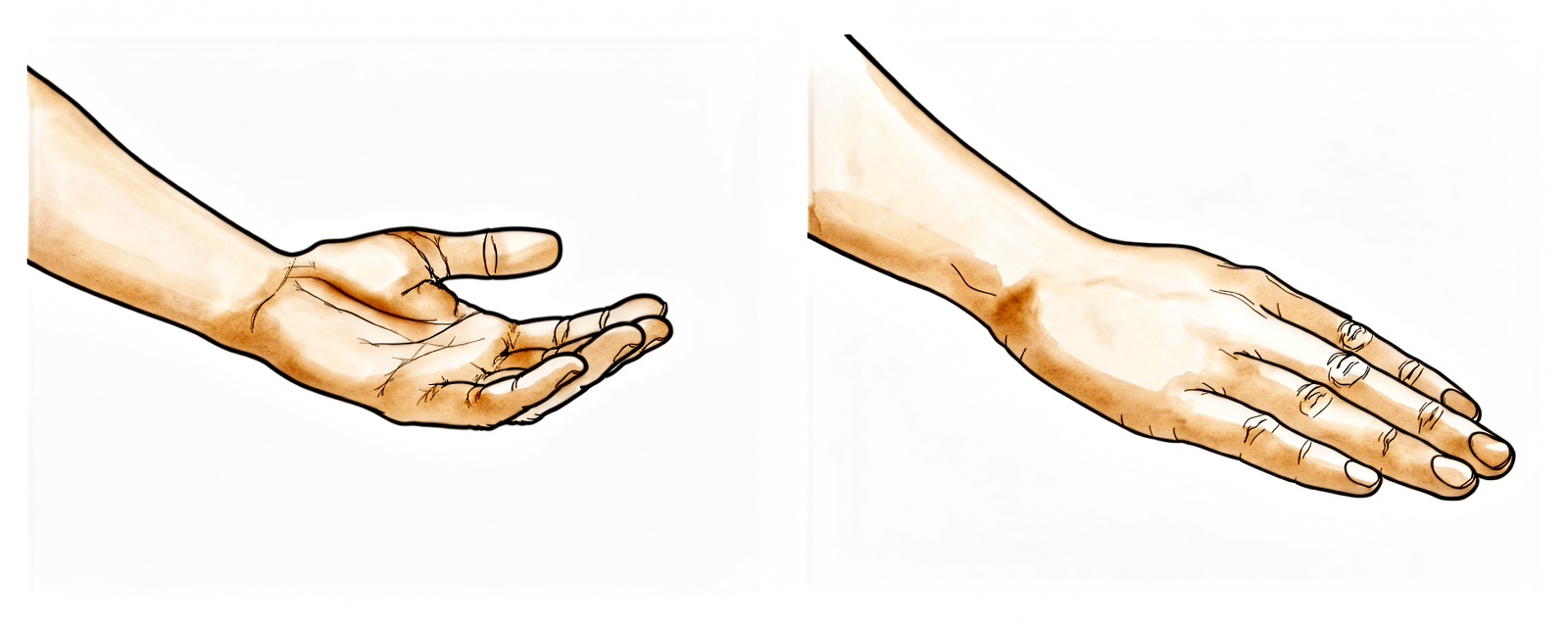
Forearm rotation (palm up / palm down)
This is the headline exercise — it is the movement the operation is designed to restore. With your elbow tucked in at your side and bent to a right angle (so your shoulder cannot cheat the movement), gently turn your palm up towards the ceiling, then slowly down towards the floor. Move only as far as is comfortable. Begin it when Dr Hirpara and your hand therapist clear you to come out of the splint for exercises — usually around two to three weeks — and make it your main focus from then on.
10 times each direction, 3-4 times a day, pain-free range
Kieran Hirpara 4.0
Wrist movement (bend and straighten)
Gently bend your wrist forwards (palm towards forearm) and backwards (back of hand towards forearm), keeping the movement slow and within comfort. This keeps the wrist from stiffening while the distal ulna settles. Keep it gentle early on and do not force the end of the range.
10 times each direction, 2-3 times a day
Kieran Hirpara 4.0
Finger movement (full fist and stretch)
Start this from day one. Make a full, firm fist, then open the hand and stretch your fingers out straight. Keeping the fingers moving early prevents stiffness and helps any swelling drain. Do it often through the day, even while your forearm is still in the splint.
10 times, every couple of hours while awake
Scar massage
Once the wound is fully healed and there are no scabs (usually from around three to four weeks), rub a small amount of plain moisturiser into the scar with firm little circles for a couple of minutes. This softens the scar and helps the skin and tendons over the distal ulna move freely. Stop if the wound is not yet fully closed.
2-3 minutes, twice a day, once the wound is healed

Kieran Hirpara 4.0
Grip and rotation strengthening (later)
A LATER exercise — only once Dr Hirpara and your hand therapist clear strengthening, commonly from around six to eight weeks. Squeeze a soft ball or putty to rebuild grip, and turn the forearm palm-up and palm-down against a light resistance (for example a light hand weight held like a hammer). Build the resistance up slowly over several weeks. Stop if turning the forearm under load is painful on the little-finger side of the wrist.
As guided by your hand therapist (from ~6-8 weeks only)
These are the exercises from your handout. Start them only as guided by Dr Hirpara and your hand therapist, staying within whatever range and limits you have been given. Finger movement starts straight away. Forearm rotation — the exercise this whole operation is built around — and wrist movement begin once you are cleared out of the splint, usually around two to three weeks, and rotation then becomes your main focus. Scar massage starts once the wound is fully healed. Grip and rotation strengthening belongs to a later phase and should not be started until you are specifically cleared. Stop anything that causes sharp pain on the little-finger side of the wrist.
Your clinical protocol¶
The rest of this page is the staged clinical protocol for rehabilitation after hemiresection-interposition arthroplasty of the distal radioulnar joint. This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. This is a joint-reshaping (arthroplasty) procedure, not a repair — there is no construct under tension to protect for months. The deliberate restraint is short: a brief splinted period to let the soft-tissue interposition and capsule settle, after which early restoration of forearm rotation is the explicit priority because rotation is the function the operation exists to restore. The principal load to respect throughout is rotational loading of the distal ulna, which is what provokes painful ulnar-stump instability and radioulnar convergence.
Prior to treatment, check the patient's operation report and past medical history, and liaise with the treating surgeon regarding any concurrent procedures (TFCC repair, distal radius osteotomy, PIN neurectomy, extensor reconstruction), the stability of the distal ulnar stump assessed intra-operatively, and the prescribed splint and rotation ceiling. A concurrent TFCC repair or distal radius osteotomy lengthens the protected phase; an isolated hemiresection for degenerative or post-traumatic arthritis follows the shorter pathway below. Dr Hirpara preserves the TFCC, ulnar styloid and ulnar soft-tissue attachments, so the distal ulna remains supported — the rehab can therefore prioritise early rotation.
Phase I — protected settling in a splint (weeks 0 to 2-3)¶
The first two to three weeks protect the soft-tissue interposition and capsule while keeping the rest of the limb mobile. The forearm rests in a splint (commonly an above-elbow / Muenster-type splint or cast that limits forearm rotation), removed only for hygiene and, towards the end of the phase, for the first gentle rotation. Fingers move from day one.
For your hand therapist:
Education and precautions - Immobilise in the prescribed splint (above-elbow / Muenster-type, or per surgeon) limiting forearm rotation; off only for hygiene and cleared exercises - No loaded forearm rotation; no weight-bearing or twisting through the operated forearm - Reassure that early grip weakness and swelling on the ulnar side are expected
Management - Wound: surgical dressings as directed; monitor for infection - Oedema: elevation, gentle hand pump, ice as needed - Exercises: active finger, thumb and (if not blocked by the splint) shoulder ROM from day one; gentle elbow ROM as the splint allows; introduce gentle pain-free active forearm rotation in the last few days of this phase if the surgeon permits early removal
Criteria to progress - Wound settling; splint period (≈2-3 weeks for isolated hemiresection) complete; cleared by surgeon for active rotation
Phase II — early forearm rotation (the priority) (weeks 2-3 to 6)¶
This is the defining phase. Out of the splint, active pronation and supination become the headline of rehabilitation — gentle, frequent, pain-free, and unloaded. Wrist motion is added. Rotation is the function the operation restores, so it is pursued actively here while loading is still withheld.
For your hand therapist:
Assessments - Active and passive forearm pronation/supination (target restoration toward the ~80° each direction reported in outcome series); wrist and finger ROM; pain on the ulnar wrist; swelling; wound/scar review
Education and precautions - Forearm rotation is the priority — frequent, pain-free, unloaded active pronation/supination, elbow tucked at the side to isolate the forearm - No resisted or loaded rotation, no heavy gripping, no twisting tasks until ~6-8 weeks - Some splints further limit end-range rotation for a few weeks after cast removal — respect any prescribed ceiling
Management - Exercises: active and active-assisted pronation/supination as the main focus; active wrist flexion/extension and radial/ulnar deviation; continue finger and grip ROM (no resisted grip yet); begin scar management once the wound is fully healed - Modalities for oedema and scar as needed
Criteria to progress - Comfortable, controlled, near-full pain-free active forearm rotation; wound healed; pain ≤3/10; no provocative ulnar-side pain on gentle rotation
Phase III — strengthening and return (weeks 6-8 and beyond)¶
Once rotation is restored and pain-free, strengthening begins and is built up gradually: grip first, then loaded forearm rotation, watching specifically for painful ulnar-stump instability or radioulnar convergence under load. Return to heavier work and sport is criterion-based.
For your hand therapist:
Assessments - Grip strength versus the other side (outcome series report recovery toward ~85-90% of the contralateral side); forearm-rotation strength and any pain or instability on loaded rotation; functional and work-/sport-specific testing as appropriate
Education and precautions - Introduce resisted grip first, then graded loaded forearm rotation (e.g. hammer turns with a light weight) from around six to eight weeks; build load slowly - Watch for painful ulnar-stump instability / radioulnar convergence under axial or rotational load — if provoked, reduce load and liaise with the surgeon
Management - Exercises: progressive grip/putty work; graded resisted pronation/supination (light → moderate); task-specific loading; continue any residual ROM work - Consider discharge once rotation and grip are functional and near-symmetrical and a suitable return of function is achieved - Consider referral back to the treating doctor if recovery plateaus, or if there is persistent ulnar-side load pain suggesting stump instability or convergence
Criteria for return to load/sport - Near-symmetrical grip and rotation strength; pain-free loaded rotation; no instability on functional testing
Getting back to work and activity¶
Light everyday hand use — eating, writing, light self-care — is encouraged from the start, within comfort, as long as it does not involve forced or loaded twisting of the forearm. Because your forearm is splinted early and you must be able to safely control the wheel (including turning it), plan for help with transport in the first few weeks; driving resumes once you are out of the splint and can comfortably and safely rotate the forearm to steer, as confirmed at your review.
Loaded twisting tasks — opening stiff jars, wringing, using a screwdriver, carrying heavy bags on that side — wait until strengthening is cleared (commonly around six to eight weeks) and are then built up gradually. Return to heavier manual work and sport follows the same criterion-based progression and depends on regaining pain-free, near-symmetrical forearm rotation and grip — judged by Dr Hirpara and your hand therapist, not by the calendar alone.
After your protocol¶
This protocol works alongside the practice's general recovery advice — see managing post-operative pain, wound care and scar management. If your DRUJ problem followed a wrist fracture, the distal radius fracture fixation protocol is a useful companion. The phased plan above reflects published rehabilitation guidance after distal radioulnar joint hemiresection arthroplasty, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your forearm progresses.
Evidence & references
DRUJ Hemiresection-Interposition Arthroplasty (Bowers) — Procedure Outcomes & Post-operative Rehabilitation¶
Topic scope: post-operative rehabilitation after hemiresection-interposition arthroplasty (HIT) of the distal radioulnar joint (DRUJ) — the Bowers procedure — for painful DRUJ arthritis (degenerative, post-traumatic, or inflammatory). The arthritic portion of the ulnar head is partially resected and a soft-tissue spacer is interposed, preserving the TFCC, ulnar styloid and ulnar soft-tissue attachments so the distal ulna remains supported. This is a joint-reshaping arthroplasty, not a repair or reconstruction: the rehab is therefore an early-rotation pathway built around a short protected settling phase, then prioritised restoration of forearm pronation/supination, then graded loading — not months of construct protection.
Defining principle of the rehab here: the operation exists to restore pain-free forearm rotation, and nothing is sutured under tension that must heal protected for months. The deliberate restraint is a brief splinted phase (commonly an above-elbow / Muenster-type splint limiting forearm rotation for ~2-3 weeks in the isolated case) to let the soft-tissue interposition and capsule settle. After that, early active pronation/supination is the explicit priority — rotation is the function the operation restores. The single load to respect throughout is rotational/axial loading of the distal ulna, which provokes the characteristic failure mode: painful ulnar-stump instability and radioulnar convergence. The main branch point that lengthens the protected phase is a concurrent procedure (TFCC repair, distal radius osteotomy, extensor reconstruction).
A. PROCEDURE OUTCOMES (hemiresection-interposition arthroplasty)¶
The Bowers HIT is a long-established, generally reliable salvage for the arthritic DRUJ. The evidence base is level IV (retrospective cohorts and case series, no randomised trials), but it is consistent across decades: most patients gain durable pain relief and improved, stable forearm rotation, with the principal residual concern being ulnar-stump instability / radioulnar convergence under load.
- The original Bowers series established the procedure and its rationale. Bowers' 1985 description (38 patients, mean ~2.5 yr) reported stable, painless rotation in the great majority — in rheumatoid patients ~85% achieved stable painless rotation (pronation ~84°, supination ~77°), and degenerative/post-traumatic patients achieved painless rotation averaging ~80° in each direction. The technique was explicitly designed to preserve the functional ulnocarpal ligament complex [Bowers, J Hand Surg Am 1985]. Level IV (foundational case series).
- Long-term outcomes are durable but with a defined complication rate. A long-term cohort (66 patients, mean follow-up 8.6 years) reported low residual pain (median NRS 1/10), an overall complication rate of ~14% and reoperation ~8%; reported complications included stylocarpal impingement, ulnar subluxation, exostoses and tendon rupture. Inflammatory-arthritis patients had lower pain than post-traumatic patients (median 0 vs 5). The same series found PIN neurectomy associated with improved pain scores [HIT long-term outcome study, Hand (N Y) 2019]. Level IV (cohort).
- Forearm rotation, grip and pain all improve measurably. A capsuloretinacular HIT series (21 wrists, mean ~2 yr 10 mo) reported significant gains: pronation 56.8°→83.0°, supination 60.0°→82.0°, grip 66.0%→87.4% of the contralateral side, VAS pain 62→23 mm, DASH 37.7→25.0, PRWE 48.1→24.4, with no post-operative DRUJ instability reported in that series [HIT capsuloretinacular series, J Wrist Surg 2023]. Level IV (cohort).
- HIT sits within a family of DRUJ salvage options (Darrach distal ulna resection, Sauvé-Kapandji arthrodesis-pseudarthrosis, matched/hemiresection variants, and ulnar-head implant arthroplasty), each with its own instability/convergence profile; HIT's selling point is preservation of the ulnar support structures to reduce stump instability versus a formal Darrach [Bowers 1985; Glowacki, Hand Clin 2005; Chidgey, JAAOS 1995; Rekant, Hand Clin 2012; Murray, Hand Clin 2011]. Mechanistic / narrative-review.
B. REHABILITATION / THERAPY EVIDENCE¶
There is no trial-level evidence for any specific rehabilitation regimen after DRUJ HIT. Protocols are surgeon- and technique-derived expert consensus, reported as the post-operative methods of the outcome series and operative-technique articles above. The consensus is consistent on its key features.
- A brief protected settling phase, not prolonged immobilisation. In the isolated hemiresection (no distal radius osteotomy, no TFCC repair), a long-arm plaster splint for ~10 days followed by a removable Muenster splint for a further 2-3 weeks is typical; cohort series report an upper-arm cast ~3 weeks then a forearm cast 1-2 weeks. Where a distal radius osteotomy or TFCC repair is added, immobilisation is longer (e.g. a long-arm cast in ~45° supination for ~4 weeks) [Pillukat & van Schoonhoven, Oper Orthop Traumatol 2009; HIT capsuloretinacular series, J Wrist Surg 2023]. Weak / expert consensus.
- Early forearm rotation is the explicit priority once protection ends. The whole point of the operation is rotation, so active pronation/supination is pursued early and frequently. Some protocols further limit end-range rotation by splint for ~4 more weeks after the cast comes off before unrestricted motion and load [Pillukat & van Schoonhoven 2009]. Weak / expert consensus.
- Loading is added last, watching for the characteristic failure mode. Range and load are returned to normal after the rotation-limited window; the specific thing to watch is painful ulnar-stump instability and radioulnar convergence under axial/rotational load, which is the biomechanically demonstrated weak point of distal-ulna procedures [Sauerbier et al., J Hand Surg Br 2002; Douglas et al., J Hand Surg Am 2014; Barret et al., Orthop Traumatol Surg Res 2020]. Mechanistic (biomechanical) + consensus.
- Finger, thumb, elbow and shoulder motion from day one is standard to prevent stiffness, as in any forearm/wrist immobilisation pathway. Consensus.
Recovery trajectory (expected, evidence-anchored)¶
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protected settling | Week 0 to 2-3 | Splint limiting forearm rotation (Muenster / above-elbow type) | Active finger/thumb/shoulder ROM from day 1; elbow ROM as splint allows; first gentle pain-free rotation toward end of phase | None through forearm | Longer if concurrent TFCC repair or distal radius osteotomy (cast in supination ~4 wk) |
| II — Early forearm rotation (priority) | Week 2-3 to 6 | Unloaded; some protocols cap end-range rotation a few more weeks | Active pronation/supination as the main focus, elbow tucked; add wrist ROM; finger/grip ROM; scar massage once healed | No resisted/loaded rotation, no heavy grip | Target restoration toward ~80° each direction; pain-free is the rule |
| III — Strengthening & return | Week 6-8+ | Restrictions lifted progressively | Resisted grip first, then graded loaded rotation (hammer turns); task-specific loading | Build load slowly; grip recovers toward ~85-90% contralateral | Watch for ulnar-stump instability / radioulnar convergence under load |
(Phase windows mirror the precautions and phase tables in the patient protocol; they are typical expert-consensus guides, not trial-derived deadlines, and lengthen with concurrent procedures.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- HIT vs Darrach. The Darrach (complete distal ulna resection) is simpler but sacrifices the ulnar support structures and is more prone to painful proximal ulnar-stump instability and radioulnar convergence, especially in younger, higher-demand or post-traumatic patients. HIT preserves the TFCC/styloid/attachments to mitigate this — but biomechanical work shows HIT also converges under load, just to a different degree, so convergence is a spectrum, not a HIT-vs-Darrach binary [Sauerbier et al., J Hand Surg Br 2002; Douglas et al., J Hand Surg Am 2014]. Darrach remains reasonable in low-demand/elderly patients. *Moderate (biomechanical
- cohort).*
- HIT vs Sauvé-Kapandji. Sauvé-Kapandji fuses the DRUJ and creates a controlled proximal pseudarthrosis, preserving the ulnar head/buttress for the carpus; it is often favoured where ulnar translation of the carpus is a concern (e.g. rheumatoid), but it too can develop painful proximal-stump instability. Long-term Sauvé-Kapandji and modified-Sauvé-Kapandji series report durable function with that caveat [Reissner et al., J Hand Surg Eur 2021; Zimmermann et al., Arch Orthop Trauma Surg 2003]. Choice is patient- and pathology-specific, not evidence-mandated. Moderate.
- HIT vs ulnar-head (implant) replacement. Implant ulnar-head arthroplasty is an alternative — particularly for failed resection/instability salvage — restoring a load-bearing buttress, but it adds implant-specific complications. Long-term implant series report good outcomes; it is increasingly used to rescue a painful, unstable stump after resection-type procedures [Kakar et al., J Hand Surg Am 2010; Adams, Hand Clin 2010; Watts et al., Hand Clin 2010; Rekant, Hand Clin 2012]. Moderate.
- The rehab regimen itself is consensus, not trial-derived. No RCT compares immobilisation length, rotation timing or loading progression after HIT. The "brief protection → early rotation → graded load" structure is inferred from technique articles and the methods of level-IV outcome series. Exact phase timings are typical, not deadlines, and shift with concurrent procedures. Weak / expert consensus.
- Patient selection drives results. Inflammatory-arthritis patients report lower residual pain than post-traumatic patients in long-term follow-up; adjunct PIN neurectomy is associated with better pain scores. Both point to outcome being substantially a selection/technique matter, not a rehab one [HIT long-term cohort, Hand 2019]. Moderate (within level-IV data).
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG (RCT / SR): none. There are no randomised trials of DRUJ HIT or of its rehabilitation.
- MODERATE: the biomechanical basis of radioulnar convergence / ulnar-stump instability under load across distal-ulna procedures (cadaveric studies); the comparative trade-offs among HIT / Darrach / Sauvé-Kapandji / ulnar-head replacement (consistent cohort + mechanistic data).
- LEVEL IV (cohort / case series — the outcome evidence): pain relief, grip recovery (~85-90% contralateral), pronation/supination gains (toward ~80° each), ~14% complication and ~8% reoperation rates, durability to ~8-9 years. Consistent but uncontrolled and surgeon-reported.
- WEAK / EXPERT CONSENSUS (the rehab regimen): the specific brief-protection → early-rotation → graded-load programme, the Muenster/above-elbow splint choice, the ~2-3 week protected window, and all exact phase timings — derived from technique articles and the methods sections of level-IV series, lengthened by concurrent procedures. No comparative rehab evidence exists.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Glowacki KA. Hemiresection arthroplasty of the distal radioulnar joint. Hand Clin. 2005. DOI: 10.1016/j.hcl.2005.08.002
- Sauerbier M, Fujita M, Hahn ME, et al. The dynamic radioulnar convergence of the Darrach procedure and the ulnar head hemiresection interposition arthroplasty: a biomechanical study. J Hand Surg Br. 2002. DOI: 10.1054/jhsb.2002.0763
- Douglas KC, Parks BG, Tsai MA, et al. The biomechanical stability of salvage procedures for distal radioulnar joint arthritis. J Hand Surg Am. 2014. DOI: 10.1016/j.jhsa.2014.03.028
- Barret H, Lazerges C, Chammas P, et al. Modification of matched distal ulnar resection for distal radio-ulnar joint arthropathy: analysis of distal instability and radio-ulnar convergence. Orthop Traumatol Surg Res. 2020. DOI: 10.1016/j.otsr.2020.07.008
- Chidgey LK. The distal radioulnar joint: problems and solutions. J Am Acad Orthop Surg. 1995. DOI: 10.5435/00124635-199503000-00005
- Murray PM. Current concepts in the treatment of rheumatoid arthritis of the distal radioulnar joint. Hand Clin. 2011. DOI: 10.1016/j.hcl.2010.10.002
- Lee SK, Hausman MR. Management of the distal radioulnar joint in rheumatoid arthritis. Hand Clin. 2005. DOI: 10.1016/j.hcl.2005.08.009
- Ozer K. Management of complications of distal radioulnar joint. Hand Clin. 2015. DOI: 10.1016/j.hcl.2014.12.003
- Zimmerman RM, Jupiter JB. Instability of the distal radioulnar joint. J Hand Surg Eur Vol. 2014. DOI: 10.1177/1753193414527052
- Rekant M. Distal ulna arthroplasties. Hand Clin. 2012. DOI: 10.1016/j.hcl.2012.08.016
- Watts AC, Hayton MJ, Stanley JK. Salvage of failed distal radioulnar joint reconstruction. Hand Clin. 2010. DOI: 10.1016/j.hcl.2010.05.004
- Kakar S, Swann R, Perry K, et al. Distal radioulnar joint implant arthroplasty: a long-term outcome analysis. J Hand Surg Am. 2010. DOI: 10.1016/j.jhsa.2010.05.010
- Adams BD. Complications of wrist arthroplasty. Hand Clin. 2010. DOI: 10.1016/j.hcl.2010.01.006
- Reissner L, Schweizer A, Unterfrauner I, et al. Long-term results of the Sauvé-Kapandji procedure. J Hand Surg Eur Vol. 2021. DOI: 10.1177/17531934211004459
- Zimmermann R, Gschwentner M, Arora R, et al. Treatment of distal radioulnar joint disorders with a modified Sauvé-Kapandji procedure: long-term outcome with special attention to the DASH questionnaire. Arch Orthop Trauma Surg. 2003. DOI: 10.1007/s00402-003-0529-5
- Nypaver C, Bozentka DJ. Distal radius fracture and the distal radioulnar joint. Hand Clin. 2021. DOI: 10.1016/j.hcl.2021.02.011
- Pillukat T, van Schoonhoven J. Die Hemiresektions-Interpositionsarthroplastik des distalen Radioulnargelenks nach Bowers [The hemiresection-interposition arthroplasty of the distal radioulnar joint]. Oper Orthop Traumatol. 2009. DOI: 10.1007/s00064-009-1913-2
DRUJ hemiresection literature (URLs)¶
- Bowers WH. Distal radioulnar joint arthroplasty: the hemiresection-interposition technique. J Hand Surg Am. 1985;10(2):169-178. https://www.jhandsurg.org/article/S0363-5023(85)80100-3/abstract (PMID: 3980927)
- Hemiresection interposition arthroplasty of the distal radioulnar joint: a long-term outcome study. Hand (N Y). 2019. DOI: 10.1177/1558944719873430. https://pmc.ncbi.nlm.nih.gov/articles/PMC8461192/
- Hemiresection capsuloretinacular interposition arthroplasty for distal radioulnar joint osteoarthritis. J Wrist Surg. 2023. DOI: 10.1055/s-0043-1771341. https://pmc.ncbi.nlm.nih.gov/articles/PMC11606672/
- Mid- to long-term functional results after Bowers' hemiresection interposition arthroplasty of the distal radio-ulnar joint. PubMed. https://pubmed.ncbi.nlm.nih.gov/35238965/
- Pillukat T, van Schoonhoven J. The hemiresection-interposition arthroplasty of the distal radioulnar joint (operative technique). Oper Orthop Traumatol. 2009. https://link.springer.com/article/10.1007/s00064-009-1913-2 (PMID: 20058126)
- Ulnar head hemiresection with interposition and extensor reconstruction — surgical technique. OrthOracle. https://www.orthoracle.com/library/ulnar-head-hemiresection-with-interposition-and-extensor-reconstruction/