PIP Joint Replacement PDF Evidence¶
A protected recovery plan after silicone replacement of the worn middle joint of a finger (the PIP joint), where the speed of starting movement depends on whether the surgeon went in from the front (palm side) or the back of the finger.
This protocol guides your recovery after replacement of the worn middle joint of a finger — the proximal interphalangeal (PIP) joint, the middle knuckle — with a flexible silicone spacer, performed by Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist — bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
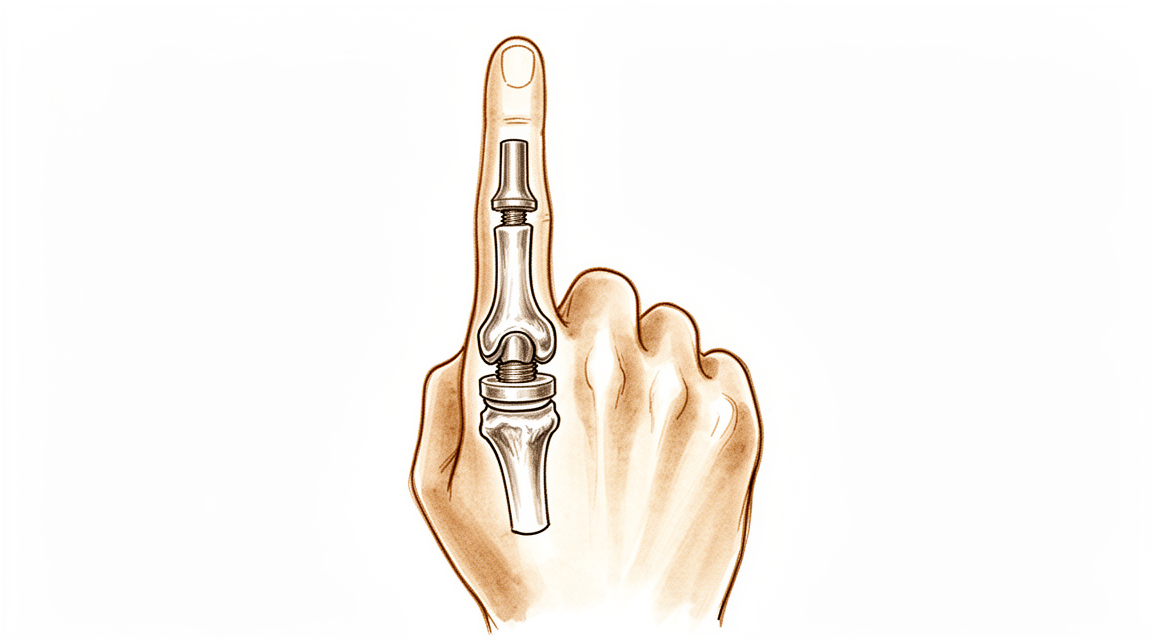
The middle joint of your finger had worn out from arthritis, which is painful and stiff. In this operation the worn joint surfaces are removed and a flexible silicone spacer (a Swanson-type implant) is placed between the two bones. The spacer is not a rigid mechanical hinge — it is a bendy spacer that holds the bones apart, lets the finger bend, and lets your own scar tissue form a new supportive sleeve around it. The main and most reliable benefit is pain relief. You should also expect a useful, modest arc of bending — usually around 40 to 60 degrees — rather than a full, normal range. Most people are very satisfied because the pain is gone and the finger is comfortable to use.
The single most important thing about your recovery is which way the surgeon went in, because that decides how soon you can move:
- From the front (the palm side — a volar approach): the straightening tendon on the back of the finger is left fully intact. Because nothing on the back has to heal, you can usually start moving the finger within a few days.
- From the back (a dorsal approach): the straightening tendon (the central slip) has to be split or lifted to reach the joint, then repaired. That repair must be protected first, so the finger is splinted straight early on and bending is introduced more gradually, under your hand therapist's guidance.
Your hand therapist will follow the plan for your surgical approach — Dr Hirpara will tell them which approach was used, and the timings below are tailored to it. Whichever approach you had, the new joint is a hinge: it likes bending and straightening in a straight line, but it does not like being pushed or twisted sideways. Protecting it from side-to-side stress is what keeps it stable for the long term.
Precautions and limitations¶
- Move the finger only in a straight line — bending and straightening — and avoid any sideways or twisting force on the operated finger. The new joint is a hinge and side stress can loosen or deform it.
- Wear your splint as directed, and use buddy strapping for activity to keep the finger tracking straight.
- If your surgery was from the back of the finger, do NOT push your own straightening beyond the limit you are given early on — the straightening tendon is healing.
- Do NOT do firm gripping, hard pinching, or heavy or twisting tasks until your hand therapist clears strengthening (commonly from around six weeks).
- Keep the other finger joints, your wrist and your shoulder moving from the start, and use the hand for light everyday tasks within comfort.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises¶
Protected active bending (PIP joint)
With your other fingers and the splint supporting the rest of the hand, gently bend and straighten the operated middle joint of the finger within the range your hand therapist has set. Keep it slow and straight — bend and straighten in a clean line, without letting the finger drift to one side. This keeps the new joint moving so it does not stiffen.
10 times, several times a day, within your set range
Active straightening (extension)
Gently straighten the operated finger out as fully and as straight as you can, then relax. If your surgery was from the back of the finger, this is the movement to protect early — your hand therapist will guide exactly how much to do and when, because the straightening tendon needs to heal first. Never force it.
10 times, several times a day, as guided
Buddy strapping
Tape the operated finger gently to the finger next to it (above and below the middle joint, not over it). The neighbouring finger acts as a splint that guides yours to bend and straighten in a straight line and stops it tipping sideways onto the new joint. Wear it for activity as advised.
Worn during light activity, as guided by your hand therapist
Kieran Hirpara 4.0
Tendon glides
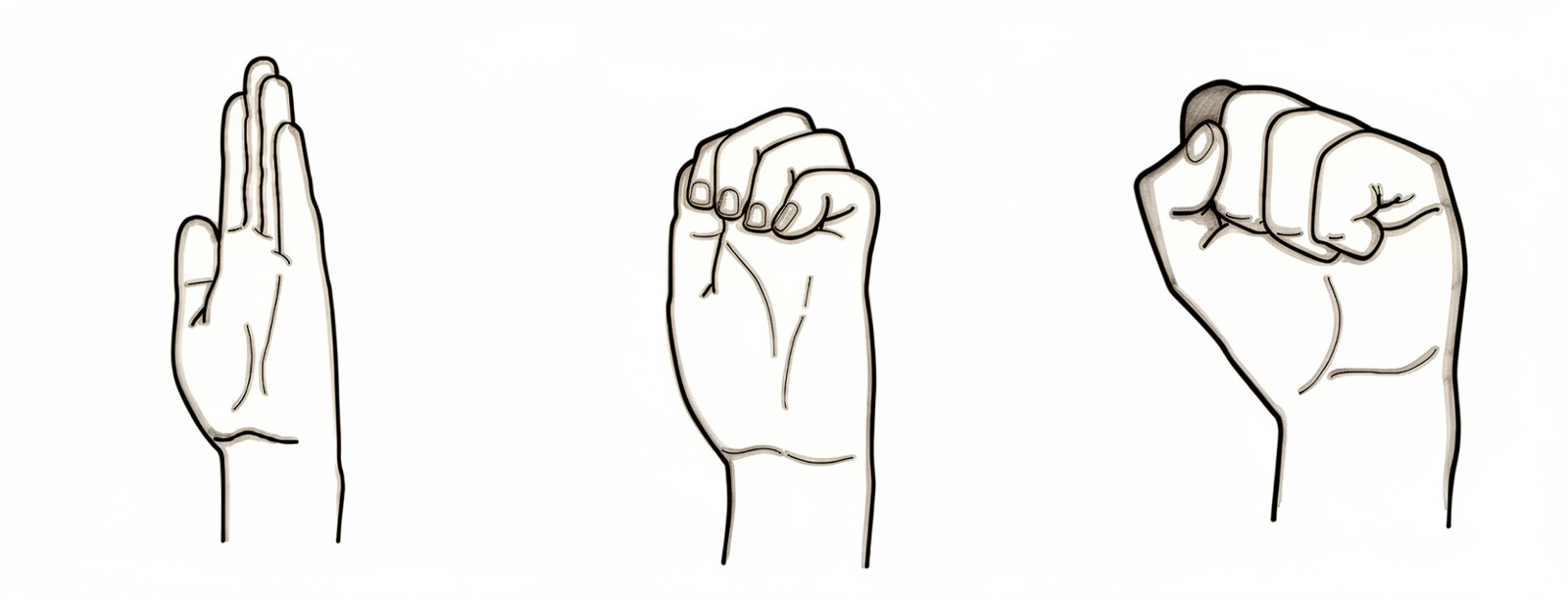
Move your hand through three shapes: fingers straight (flat hand), then bend only the end two joints into a hook, then curl into a gentle full fist, then straighten out again. This glides the tendons so they do not stick down as the finger heals. Stay within any bending limit you have been given.
5–10 times through the sequence, several times a day
Scar massage
Once the wound is fully healed, massage the scar with a little plain cream, using small firm circles for a few minutes. This keeps the scar soft and stops it tethering to the tendon and joint underneath. Do not start until your hand therapist confirms the wound has healed.
A few minutes, 2–3 times a day, once the wound is healed

Kieran Hirpara 4.0
Grip strengthening
A LATER exercise — only once your hand therapist clears strengthening (commonly from around six to eight weeks). Gently squeeze a soft ball or putty, building up slowly. Avoid hard pinching or any twisting that puts side-to-side force on the new joint until you are told it is safe.
As guided by your hand therapist (later phase only)
These are the exercises from your handout. Start them only as guided by Dr Hirpara and your hand therapist, staying within whatever range and limits you have been given. The early work keeps the finger moving in a straight line without side stress — protected bending, gentle straightening, buddy strapping and tendon glides. If your surgery was from the back of the finger, the active straightening exercise is the one to protect early and build up slowly. Grip strengthening belongs to a later phase and should not be started until you are specifically cleared. Stop anything that causes sharp pain or makes the finger feel unstable.
Your clinical protocol¶
The rest of this page is the staged clinical protocol for rehabilitation after silicone PIP joint arthroplasty. This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. The protocol is approach-dependent, and this is the central branch point: a volar (palmar) approach leaves the extensor mechanism intact and permits early active motion within days; a dorsal approach divides or splits the central slip, so extensor healing must be protected first with extension orthotics and graded flexion. Throughout, the silicone implant is a flexible spacer whose long-term stability depends on the peri-implant capsule — so coronal (lateral) stress is avoided and motion is kept in a pure sagittal arc.
Prior to treatment, confirm with the treating surgeon the surgical approach (volar vs dorsal), the integrity/repair of the central slip and collateral ligaments, and any intra-operative arc. Dr Hirpara will specify the approach; select the volar (early-active-motion) or dorsal (extension-protected) pathway accordingly. The expected functional target is a pain-free arc of roughly 40–60°, not full range.
Phase I — protect and initiate motion (weeks 0 to 3)¶
The first weeks protect the soft tissues while preventing stiffness, with the pace set entirely by the approach. The implant is stable in flexion–extension but vulnerable to side load, so all motion is kept in a clean sagittal plane and the finger is supported by buddy strapping and a splint.
For your hand therapist:
Education and precautions - Identify the surgical approach and follow the matching pathway: - Volar approach: extensor mechanism intact → begin active PIP/DIP motion at 3–5 days. Fit a volar extension-block / template splint permitting a short flexion arc (commonly ~30° initially), increased progressively. - Dorsal approach (central slip split/repaired): protect extension. PIP splinted near full extension full-time; introduce active flexion in a limited short arc under supervision, respecting the central-slip repair. (A relative-motion / dynamic-extension scheme may be used per surgeon preference.) - Strict avoidance of coronal (lateral/radial–ulnar) stress on the operated joint — buddy strap to the adjacent digit to guide pure sagittal tracking. - No gripping, pinching or resisted/loaded use.
Management - Wound: surgical dressings as directed; monitor for infection - Oedema: elevation, gentle retrograde massage, light compressive wrap - Exercises: protected active PIP/DIP flexion–extension within the set arc; tendon glides; active motion of uninvolved joints (DIP, MCP, wrist, thumb); commence buddy strapping for activity - Splint worn full-time between exercise sessions
Criteria to progress - Wound healing satisfactorily; no extensor lag developing (dorsal pathway); comfortable, controlled motion within the current arc
Phase II — advance motion (weeks 3 to 6)¶
The flexion arc is opened up and, for dorsal-approach fingers, the extension protection is progressively relaxed as the central slip consolidates. The goal of this window is to bank the useful arc (≈40–60°) before scar maturation fixes the range.
For your hand therapist:
Assessments - Active and passive PIP arc; extensor lag (dorsal pathway); coronal stability; pain and oedema; wound/scar review
Education and precautions - Progressively increase the permitted flexion arc toward the functional target (≈40–60°) - Volar: advance active flexion as tolerated; add gentle passive flexion if extension is full and stable - Dorsal: wean extension splinting per central-slip healing (commonly weaning daytime support across weeks 4–6); guard against extensor lag — do not chase flexion at the cost of active extension - Continue strict avoidance of lateral/torsional load; no resisted strengthening yet
Management - Exercises: graded active and active-assisted PIP flexion–extension; blocking exercises to focus PIP motion; continue tendon glides and buddy strapping; commence scar massage once the wound is healed - Maintain full motion of adjacent joints
Criteria to progress - Healed wound; stable joint in the coronal plane; functional pain-free arc established; minimal extensor lag (dorsal)
Phase III — strengthen and return (weeks 6 to 12 and beyond)¶
Once motion is established and the soft tissues are sound (around six weeks), light strengthening begins and is built up gradually. Strengthening is kept axial — grip and straight-line loading — while lateral/torsional stress on the implant is still respected long-term.
For your hand therapist:
Assessments - Grip and pinch versus the other side; final PIP arc; coronal stability; functional and task-specific testing
Education and precautions - Begin light grip strengthening from around six weeks, building gradually - Introduce pinch loading cautiously and continue to avoid forceful lateral/twisting loads on the operated joint indefinitely (implant longevity) - Set realistic expectations: durable pain relief is the primary gain; the final arc is modest (≈40–60°) and largely set by ~3 months
Management - Exercises: progressive grip/putty work; graded functional and work-specific loading; continue any residual mobility and scar work - Consider discharge once a stable, comfortable, functional finger with a useful pain-free arc is achieved - Refer back to the treating doctor if recovery plateaus, the joint becomes unstable/deviates, or implant failure is suspected
Criteria for discharge / return - Comfortable, pain-free, coronally stable joint with a functional arc; adequate grip; able to meet daily and work demands
Getting back to work and activity¶
Light everyday hand use — eating, writing, light self-care — is encouraged from the start, within comfort, as long as it stays in a straight line and avoids side-to-side or twisting force on the operated finger. Driving is usually possible once you can grip the wheel comfortably and control the car safely, you are out of any restrictive splint, and you are no longer taking strong pain medication — typically a couple of weeks, and confirmed at your review.
Firmer gripping and loaded tasks wait until about six weeks, and are then built up gradually. Heavier manual or twisting work is the last thing to return, and is based on regaining a comfortable, stable finger with adequate grip — judged by Dr Hirpara and your hand therapist, not by the calendar alone. Remember the lasting deal with this operation: reliable pain relief and a useful arc of around 40 to 60 degrees, with side-to-side stress on the joint avoided for the long term to protect the implant.
After your protocol¶
This protocol works alongside the practice's general recovery advice — see managing post-operative pain, wound care and scar management. The phased plan above reflects published rehabilitation guidance after silicone PIP joint arthroplasty, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to which surgical approach was used and how your finger progresses.
Evidence & references
Silicone PIP Joint Replacement — Procedure Outcomes & Post-operative Rehabilitation (Swanson-type Arthroplasty for PIP Osteoarthritis)¶
Topic scope: post-operative rehabilitation after silicone (Swanson-type) proximal interphalangeal (PIP) joint arthroplasty for primary osteoarthritis. The worn joint surfaces are excised and a flexible silicone spacer is implanted; this is an interposition / encapsulation arthroplasty, not a rigidly-fixed mechanical hinge. The implant works as a flexible spacer around which a peri-implant fibrous capsule forms to provide stability. The dominant, reliable benefit is pain relief; the functional gain is a modest active arc (~40–60°), not restoration of normal range.
Defining principle of the rehab here: the rehabilitation pathway is dictated by the surgical approach, because the rate-limiting tissue is the extensor mechanism, not the implant. A volar (palmar) approach leaves the central slip and extensor mechanism intact → it permits immediate / early active motion (within 3–5 days). A dorsal approach must split or reflect the central slip to reach the joint → the extensor repair must be protected first with extension orthotics and a graded, short-arc flexion programme. Across both pathways the silicone spacer is stable in the sagittal (flexion–extension) plane but vulnerable in the coronal plane, so the programme deliberately avoids lateral / torsional load and tracks the joint in a pure sagittal arc (buddy strapping). Therapy aims to bank the useful arc before scar maturation fixes it while protecting extension and the implant — it is not an immobilise-to-heal construct in the volar case.
A. PROCEDURE OUTCOMES (silicone PIP arthroplasty for osteoarthritis)¶
Silicone PIP arthroplasty is a reliable pain-relieving operation with predictable but modest motion; the principal debates are over surgical approach and implant choice (silicone vs surface-replacement/pyrocarbon), not whether arthroplasty relieves pain.
- Pain relief is high and durable; motion gains are modest. A long-term series of Swanson silicone PIP arthroplasty for osteoarthritis (mean ~10-year follow-up) reported excellent pain relief (mean VAS ~0.4) with essentially unchanged arc (≈55° pre-op → ≈50° post-op) and high patient satisfaction — patients would have the surgery again despite limited motion gain [Bales, Wall & Stern, J Hand Surg Am 2014]. Moderate (level-IV long-term cohort).
- The volar approach can improve the active arc. A volar-approach silicone PIP series reported the active arc improving from ~33° to ~72°, with good function and satisfaction, by preserving the extensor mechanism and enabling early motion [Proubasta et al., J Hand Surg Am 2014]. Moderate–weak (level-IV).
- Radiographic implant deformation/fracture is common but poorly correlated with symptoms. In the long-term Swanson series most implants deformed and many fractured radiographically, yet clinical revision was uncommon (survivorship ~90% at ~10 years) and there was no correlation between radiographs and satisfaction [Bales, Wall & Stern 2014]. Strong natural-history signal within a cohort.
- Silicone vs surface-replacement and pyrocarbon implants give broadly comparable clinical results; no implant is clearly superior. Systematic review across implants/approaches found comparable outcomes with implant-/approach-specific complication profiles [Yamamoto et al., Plast Reconstr Surg 2017; Carlson Strother, Moran & Rizzo, JAAOS 2023]. Moderate (SR + narrative review).
- Pyrocarbon and resurfacing implants carry their own failure modes (subsidence, squeaking, intra-operative periprosthetic fracture, instability), informing implant choice rather than rehab [Watts et al., J Hand Surg Am 2012; Wagner et al. medium-term 2018 & intra-op fractures 2015; Branam et al. resurfacing-vs-silicone 2007]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE¶
The central rehab questions are (1) how soon to move and (2) how to splint, and the answer to both is set by the surgical approach and the extensor mechanism. The evidence base is low-level (expert consensus / single-cohort therapy series) — there are no RCTs comparing PIP arthroplasty rehab pathways.
- Approach dictates the timeline (the core principle). Surgical reviews establish that a volar approach preserves the central slip and permits immediate active and passive motion, while a dorsal approach requires post-operative protection of the split/repaired central slip before flexion is advanced [Renfree, Bone Joint J 2022 (surgical approaches); Herren, Hand Clin 2017; Yamamoto et al. 2017]. Moderate (surgical evidence) — strong mechanistic basis.
- A structured 12-week, splint-based therapy programme is the consensus framework (dorsal pathway). Feldscher's hand-therapy protocol for PIP (pyrocarbon, central-slip-splitting dorsal approach) uses a volar static finger orthosis allowing a limited short-arc PIP/DIP active arc that is increased over the rehab course, with a hand-based resting splint (MCP flexed, PIP/DIP near 0°) for full-time use except during template-splint exercise [Feldscher, J Hand Ther 2010]. Weak (expert-consensus protocol).
- A defined controlled-motion program exists and reports good arcs. A controlled-motion rehabilitation program for PIP arthroplasty reported favourable range-of-motion outcomes, supporting graded controlled motion over rigid immobilisation [Ramanathan, Koludrovich & Evans, J Hand Ther 2021]. Weak (cohort / programme description).
- Static and dynamic extension splinting give similar results. A comparison of static vs dynamic splinting after PIP pyrocarbon arthroplasty found comparable outcomes, favouring static splinting for simplicity and patient convenience [Jennings & Livingstone / static-vs-dynamic cohort, J Hand Ther 2011]. Weak–moderate (comparative cohort).
- Coronal-plane protection is the durable, lifelong caveat. Collateral integrity and avoidance of lateral stress underpin long-term implant stability; collateral compromise drives instability/deviation [Carlo et al., collateral reconstruction, J Hand Surg Am 2016; Carlson Strother et al. 2023]. Consensus / mechanistic.
Recovery trajectory (expected, evidence-anchored)¶
| Phase | Window | Restraint (by approach) | Hand-therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect & initiate motion | Week 0–3 | Volar: active motion at 3–5 days, short flexion arc (~30°) in template/extension-block splint. Dorsal: PIP splinted near extension full-time; supervised short-arc flexion only | Protected sagittal PIP/DIP motion; tendon glides; buddy strapping; uninvolved-joint motion; no lateral/torsional load | None (no grip/pinch) | Implant stable in flexion–extension, vulnerable coronally |
| II — Advance motion | Week 3–6 | Progressively increase flexion arc toward ~40–60°. Dorsal: wean extension splint as central slip consolidates (≈wk 4–6); guard against extensor lag | Graded active/AAROM flexion–extension; blocking; scar massage once healed; continue buddy strapping | Still no resisted strengthening | Bank the useful arc before scar maturation fixes it |
| III — Strengthen & return | Week 6–12+ | Lifting/grip restrictions progressively lifted; lateral/twisting load avoided indefinitely | Light grip → cautious pinch; functional & work-specific loading | Grip from ~6 wk, graded | Pain relief is the durable gain; final arc (~40–60°) largely set by ~3 months |
(Phase windows mirror the precautions in the patient protocol; they are typical guides — not trial-derived deadlines — and the volar vs dorsal split is the dominant variable.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Volar vs dorsal approach (the rehab-defining question). The volar approach spares the extensor mechanism and permits early active motion (and a better reported arc), at the cost of being more technically demanding; the dorsal approach is more familiar but mandates extensor protection and a slower, splint-led flexion programme. Choice is surgeon-dependent and drives the entire rehab pathway. Moderate surgical evidence; no head-to-head rehab RCT.
- Implant choice (silicone vs surface-replacement vs pyrocarbon). No implant is clearly superior on clinical outcomes; silicone is durable for pain relief with high radiographic deformation/fracture that poorly predicts symptoms, while pyrocarbon/resurfacing trade different complication profiles (subsidence, instability, intra-operative fracture). Moderate (SR + cohorts).
- Static vs dynamic splinting (dorsal pathway). Comparable outcomes; static splinting is favoured for simplicity and convenience. Weak–moderate.
- Motion gain is modest and that is expected, not failure. Patients reliably lose pain but gain little arc (especially via dorsal/silicone); mislabelling the modest arc as a poor result misframes a successful pain-relieving operation. Counsel the ~40–60° expectation up front. Strong natural-history signal.
- Lifelong coronal-stress avoidance. Long-term stability depends on the peri-implant capsule and collaterals; forceful lateral/twisting load risks deviation, instability and implant failure. Consensus.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG (mechanistic / natural-history): the surgical-approach principle (volar preserves extensor mechanism → early motion; dorsal splits central slip → protect extension first); the modest-arc / reliable-pain-relief outcome pattern; radiographic implant deformation poorly predicting symptoms.
- MODERATE: procedure outcomes are level-IV case series (long-term Swanson silicone series; volar approach series); implant-comparison systematic review/narrative review; surgical-approach reviews.
- WEAK / EXPERT CONSENSUS: the specific rehabilitation regimen — short-arc controlled motion, 12-week splint-based programme, static-vs-dynamic splinting equivalence, exact phase timings. These are low-level, expert-consensus / single-cohort therapy descriptions, not trial-derived; individualise to the operative approach and tissue quality.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2014. DOI: 10.1016/j.jhsa.2013.11.008
- Proubasta IR, Lamas CG, Natera L, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014;39(6). DOI: 10.1016/j.jhsa.2014.03.033
- Weistra K, Kan HJ, van Alebeek VAHJ, et al. Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex in 72 cases. HAND. 2022. DOI: 10.1177/15589447221122829
- Branam BR, Tuttle HG, Stern PJ, et al. Resurfacing arthroplasty versus silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2007. DOI: 10.1016/j.jhsa.2007.04.006
- Yamamoto M, Malay S, Fujihara Y, et al. A systematic review of different implants and approaches for proximal interphalangeal joint arthroplasty. Plast Reconstr Surg. 2017. DOI: 10.1097/prs.0000000000003260
- Renfree KJ. Surgical approaches for proximal interphalangeal joint arthroplasty. Bone Joint J. 2022;104-B(12). DOI: 10.1302/0301-620x.104b12.bjj-2022-0946
- Herren DB. Current European practice in the treatment of proximal interphalangeal joint arthritis. Hand Clin. 2017. DOI: 10.1016/j.hcl.2017.04.002
- Carlson Strother CR, Moran SL, Rizzo M. Small joint arthroplasty of the hand: an update on indications, outcomes, and complications. J Am Acad Orthop Surg. 2023;31(15). DOI: 10.5435/jaaos-d-23-00034
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. DOI: 10.1016/j.jht.2009.10.011
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. DOI: 10.1016/j.jht.2019.04.003
- Watts AC, Hearnden AJ, Trail IA, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: minimum two-year follow-up. J Hand Surg Am. 2012. DOI: 10.1016/j.jhsa.2012.02.012
- Wagner ER, Weston JT, Houdek MT, et al. Medium-term outcomes with pyrocarbon proximal interphalangeal arthroplasty: a study of 170 consecutive arthroplasties. J Hand Surg Am. 2018. DOI: 10.1016/j.jhsa.2018.06.020
- Wagner ER, Van Demark R, Kor DJ, et al. Intraoperative periprosthetic fractures in proximal interphalangeal joint arthroplasty. J Hand Surg Am. 2015. DOI: 10.1016/j.jhsa.2015.06.101
- McGuire DT, White CD, Carter SL, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: outcomes of a cohort study. J Hand Surg Eur Vol. 2011;37(6). DOI: 10.1177/1753193411434053
- Carlo J, Dell PC, Matthias R, et al. Collateral ligament reconstruction of the proximal interphalangeal joint. J Hand Surg Am. 2016;41(1). DOI: 10.1016/j.jhsa.2015.10.007
- Aversano FJ, Calfee RP. Salvaging a failed proximal interphalangeal joint implant. Hand Clin. 2018. DOI: 10.1016/j.hcl.2017.12.011
PIP arthroplasty rehabilitation literature (URLs)¶
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. https://pubmed.ncbi.nlm.nih.gov/20036511/
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. https://pubmed.ncbi.nlm.nih.gov/31481342/
- Static versus dynamic splinting for proximal interphalangeal joint pyrocarbon implant arthroplasty: a comparison of current and historical cohorts. J Hand Ther. 2011. https://pmc.ncbi.nlm.nih.gov/articles/PMC3143198/
- Proubasta IR, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24799141/
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for PIP joint osteoarthritis. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24559624/
- The dorsal approach to silicone implant arthroplasty of the proximal interphalangeal joint. J Hand Surg Am. 2007. https://www.sciencedirect.com/science/article/abs/pii/S0363502307004662
- Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex. HAND. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC10953532/